|
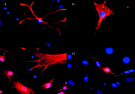
Stem cells that help mice regain
movement differentiate into many types of nervous system
cells.
Photo by John D.
Gearhart
|
|
"I was surprised by the findings, but have always thought that
these stem cells are amazing and that they represent a great
potential strategy," says Kerr who reported his findings in
November 2000 at the annual Society for Neuroscience meeting in
New Orleans.
Kerr and his colleague, Hopkins neurologist Jeffrey Rothstein,
say the results are promising step toward using the cells to
restore movement in patients with paralyzing illnesses and
injuries, such as amyotrophic lateral sclerosis (Lou Gehrig's
disease).
The researchers caution, however, that clinical use of stem cells
for motor neuron conditions is years away. Many unanswered
questions remain, such as: What mechanism explains how the cells
helped the mice regain movement? And, would stem cell injections
have lasting effects or need to be repeated?
Until recently, researchers studying neural stem cells have
focused on conditions such as Parkinson's disease or stroke,
which affect a smaller, circumscribed group of neurons. Directing
stem cells to more diffusely damaged regions of the nervous
system was presumed to be a bigger challenge.
Kerr and Rothstein hypothesized that the cerebrospinal fluid, the
nutrient soup that bathes the spinal cord, might be a means of
delivering stem cells to damaged neurons. So working with stem
cell biologists John D. Gearhart, at Hopkins, and Evan Snyder, at
Harvard University, they created injections containing neural
stem cells from mice. They injected the cells into mice infected
with a virus that causes paralysis and may serve as a model of
paralyzing conditions in people.
Did the stem cells get into the spinal cord? Kerr dissected the
mice, which were sacrificed at the end of the experiment.
"Absolutely, they made a beeline to it," he says. Thirty percent
of the stem cells had migrated into the spinal cord of the
infected mice, to a region called the ventral horn, which
contains neurons that extend processes to the muscles controlling
limb motion.
About one-third of the cells that made their way into the spinal
cord appeared to have become some type of primitive neuron. "But
they are clearly not motor neurons," says Rothstein. So how did
they help the mice regain movement? The cells may have
differentiated into supporting cells called astrocytes, which
supply hormones and other vital factors to motor neurons,
Rothstein suggests.
Curiously, the stem cells did not enter the spinal cord of
healthy animals that served as controls. "There is some signal
that has to do with motor neurons dying that serves as a
trigger," posits Kerr. "It's fascinating to see."
The researchers, who received funding from Project ALS and the
Muscular Dystrophy Association, next plan to expand their study
and to test the effects of a variety of different types of neural
stem cells. --Melissa Hendricks
|



 With a five-year $7.8 million grant from the NIH, Johns Hopkins
Medicine recently established the Center for Complementary and
Alternative Medicine (CAM), which will sponsor lab and clinical
research on alternative forms of cancer treatment, and train
physicians and medical students. Adrian Dobs (pictured at
right) is a principal investigator at the center and
professor
of endocrinology.
With a five-year $7.8 million grant from the NIH, Johns Hopkins
Medicine recently established the Center for Complementary and
Alternative Medicine (CAM), which will sponsor lab and clinical
research on alternative forms of cancer treatment, and train
physicians and medical students. Adrian Dobs (pictured at
right) is a principal investigator at the center and
professor
of endocrinology.