|
|
NOVEMBER 1999 CONTENTS
|
Vital Signs
 |
Seeing the light |
|
Cocaine's lingering effects |
|
He says, she says |
|
Still the one... |
|
War stories from the slopes |
|
A united effort in East Baltimore |
|
Public health major takes off |
|
Vital Signs
|
|
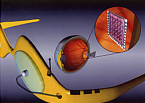
Seeing the light Points of light. Shapes. Shadows. Colors. Letters of the alphabet--all have been seen by people who are completely blind. Electronic retinal implants being developed at Hopkins's Wilmer Eye Institute are on the leading edge of research that could offer limited vision to people blinded by such eye diseases as retinitis pigmentosa and age-related macular degeneration. The technology: a computer chip prosthesis implanted near the eye's retina. If successful, such biochips would mark one of the first major scientific links between computers and neurons in the body. "Medicine and microelectronics are two fields that have made quantum leaps in recent decades," says Hopkins researcher Mark Humayun, "but they are like two gigantic towers with no bridge between. We are trying to link the two." Humayun, a retinal surgeon and biomedical engineer, and Hopkins retinal surgeon Eugene de Juan Jr. first tested the electronic stimulation of retinal neurons on a human subject at Duke University in 1992. Their patient, a blind, 71-year-old former welder, Harold Churchey, reported seeing light after the doctors used an electrode to jolt untapped neurons into sending signals to the brain. A few years later at Hopkins, Churchey reported seeing dots of light in the shape of an H, much like an H on an electronic scoreboard. At Hopkins, Humayun and de Juan have tested an implanted biochip on 15 patients, who have reported seeing points of light, shapes, and contrasts between light and dark. The testing on human patients has broken new ground in retinal research. Other teams of scientists, surgeons, and electrical engineers in the United States and Germany are working on the technology needed to stimulate the eye's unused neurons. Humayun and de Juan began their research back in the early 1990s, when they discovered that patients with some eye diseases continued to harbor an array of healthy retinal neurons, even after they'd been robbed of the photoreceptors in their eyes--the rods and cones that convert images into electric impulses. Humayun wondered: "Is there a way to jumpstart these remaining awaiting neurons and thus create the sensation of vision?" The best candidates: people with retinitis pigmentosa (RP) or age-related macular degeneration (AMD). Over 300,000 Americans have AMD, and one in 4,000 suffers from RP. In these diseases, the bipolar cells and nerve fiber layers of the retina remain healthy. By contrast, people suffering vision loss due to diabetes, glaucoma, and other diseases would not benefit because resulting damage to the optic nerve blocks signals between the eye and the brain. Researchers caution that so far only limited vision would likely be restored by the microelectronic prosthesis being developed now--mostly the perception of shapes, movements, and contrasts of light. "It's a first step," Humayun says. "The brain can fill in gaps and adjust to a lot." With the Hopkins device, an external camera mounted in the frame of a patient's eyeglasses would capture an image and convert it into an electrical signal. That signal would be wirelessly transmitted to a flexible silicon biochip, embedded with electrodes, that had been surgically attached near the retina. The chip would then electronically stimulate the healthy cells of the retina, which would send signals conveying the image to the brain's visual regions. The working title for the device: a Multiple-unit Artificial Retina Chipset (MARC). The next step for Humayun and de Juan is to create a prototype that can be implanted in patients for hours, days, or months. That's a daunting goal, partly because the implant could tear the retina's wet-tissue-paper-thin surface, or be rejected by the body. The Hopkins researchers are now testing a prototype in animals, and expect to create a device for testing in humans in two to three years. There is hope that actual implants could be used within the decade, or sooner. --Joanne Cavanaugh Simpson
|
|
Cocaine's lingering effects Singer Jackson Browne had it right when he lamented, "Cocaine, running all 'round my brain." Chronic cocaine users suffer persistent neurological deficits, says Hopkins neurologist Karen Bolla. In one of the first studies to examine the long-term effects of cocaine on the brain, Bolla found that cocaine users scored significantly lower on tests of decision making, long-range planning, memory, visual-perception skills, and manual dexterity. "We established a dose-response relationship," says Bolla. The more cocaine a person had been using, the sharper was the decline in thinking. Two grams of cocaine per week appeared to be the breakpoint. Volunteers who used more than that amount had serious impairments. Bolla and her colleagues administered the tests to 30 cocaine users who were using the drug at least four times per month and had been users for at least one year. The volunteers did not use any drugs during the study period, which consisted of a 30-day inpatient stay. The researchers also administered the tests to 21 non-drug-using control subjects. Other studies have indicated that cocaine damages the prefrontal cortex, says Bolla. If that is the case, it could explain why cocaine users have such a hard time kicking the habit. "The prefrontal cortex controls your ability to inhibit bad behavior, and is involved in goal-planning and executive skills," says Bolla. So damaging this area, she says, "makes it harder to inhibit the bad behavior." --Melissa Hendricks
Patients rate visits to physicians as more participatory when the physician is female or of the same race as the patient, according to a recent study led by Johns Hopkins researchers. In telephone surveys conducted between November 1996 and June 1998, researchers asked over 1,800 adults questions about their level of involvement during recent medical visits. Questions such as, "If there were a choice between treatments, how often would this doctor ask you to help make the decision?" and "How often does this doctor ask you to take some responsibility for your treatment?" led to the finding that patients find communication easier with female and same-race doctors. "Our study suggests that patients' satisfaction level is highly correlated with how much physicians involve them in the decision-making process," says Lisa Cooper-Patrick, lead researcher for the study and an assistant professor at the School of Medicine. "Patients who feel a greater sense of partnership with their physician are more satisfied and often see better medical outcomes." Cooper-Patrick says the study points out the need for better cross-cultural communication training for physicians, and for equipping patients to feel more comfortable dealing with their doctors. The study, reported in the August 11 issue of the Journal of the American Medical Association, also found that middle-age patients (age 40 to 65) rate their visits as more participatory than younger patients (under 30). Education also appeared to play a role: those with a graduate education said they had more participatory visits than those with a high school education or less, as did patients with better ratings of their own health status. And patients who had known their physician for three years or longer also rated their visits as more participatory than those who had known their physician for less than one year. In the next phase of the study, during which researchers will place audiotape recorders in doctors' offices during medical visits, Cooper-Patrick and colleagues will examine more closely the interplay between race and communication. --Barbara J. Kiviat '01
For the ninth year in a row, Johns Hopkins Hospital has been named No. 1 in the nation in the annual ranking conducted by U.S. News and World Report. This year, the magazine's July 19 issue ranked 188 qualifying hospitals (up from 132 last year), and placed just 13 on its "Honor Roll." Hopkins also ranked in the top tier in 14 of the 16 specialty categories listed by the newsweekly.
|
|
War stories from the slopes If you're out on the ski slopes this winter and you take a spill, pick yourself up, dust yourself off--then log onto to www.injury-study.org to share the particulars of your mishap. Researchers at Public Health's Center for Injury Research and Policy have launched the website to collect data directly from thousands of skiers and snowboarders worldwide who become injured on the slopes. The goal: "to provide an abundance of new information on steps the individual skier or snowboarder can take to prevent an injury," says epidemiologist Jeffrey Hadley. The most pertinent results will be updated weekly and posted on the website. --Sue De Pasquale
|
|
A united effort in East Baltimore Serious health problems plaguing neighborhoods within blocks of Johns Hopkins Hospital have long been a concern to many. Just outside the doors of labs where scientists are searching for vaccines for AIDS and other illnesses, the rate of sexually transmitted diseases in East Baltimore is the highest in the country. A Hopkins-based report released by the President's Council on Urban Health this year made 18 recommendations to help battle the East Baltimore community's health woes. The council, convened by Hopkins President William R. Brody, drew its more than 100 members from every local division of the university, and tapped community leaders, including Police Commissioner Thomas Frazier. One of the council's top priorities for Hopkins--after the goals of expanding treatment for substance abuse and pushing for economic growth--is the establishment of an Urban Health Institute. The planning is being overseen by Provost Steven Knapp. In part, the Hopkins-based institute would act as a clearinghouse of information about university research and community health programs, and--led by an executive director and staff--monitor how the programs can work together and how patients can be better guided to the right source for help. The goal is to create a singular vision for battling the area's problems. "We don't think anyone really has a true handle on how much research is going on," says Colene Daniel, a Hopkins Health System vice president who co-chairs the council with Martha Hill, professor of nursing. "There are hundreds of millions of dollars of research and it is not coordinated." The institute also would act as a community liaison--for the first time giving Hopkins such a centralized point of contact. Other proactive missions could include analyzing health policies on the state or federal level and raising money for health-oriented projects. For the community, there would be one source to contact with questions, concerns, or advice about health-related issues. The liaison is a key part of an effort to address the distrust of some East Baltimore residents, who have complained that the hospital hasn't done enough to ease problems in the blocks surrounding the hospital. While Hopkins does provide health services to residents, the health problems in Baltimore, as in many American urban areas, have so far proven insurmountable. City health department statistics show that East Baltimore has the city's highest age- and sex-adjusted rates of mortality from cardiovascular disease. Residents also suffer from high rates of diabetes, cancer, HIV-related illnesses, substance abuse, and health problems linked to violence. Even more alarming, the rate of syphilis has been the highest of any city in the developed world. The next phase for the institute includes nationwide searches for an executive director and funding sources, as well as the hiring of staff. A budget for the institute has not yet been determined. But the initiative overall appears to be on the fast track: "We hope to have people recruited and in place by next July," Daniel says. "But that's a hope." --JCS
Move over Biology. Watch out International Relations. Public Health is gaining "major" ground among Hopkins undergraduates-- and quickly. "We've had a public health major [here] since the 1970s, but in the last three to four years it's boomed," says Jim Goodyear, associate director of the public health studies program. "It sort of caught us all unaware." This spring, some 85 Hopkins seniors will graduate with a major in public health. That's up from 45 last year, and an average of 20 in previous years. "We don't know where the natural ceiling is on this," says Goodyear. "I don't think that we're there yet. There's still room for growth." Until recently, public health was "primarily a premed major," Goodyear says. But that's changing, too. Of last year's graduating public health majors, roughly a quarter went on to graduate schools of public health--twice the number of majors who went on to medical school, says Goodyear. The major is appealing to students who are "community minded, service-minded--who want to be out in the field working with people," he says, then adds, "There are a fair number of international students in the major--students who have a sense of the world as a globe." Says senior Mary Pohl '00, founder of the Public Health Students' Forum, "I came into Hopkins wanting to be a physician. Public health has really opened my eyes to the social problems and social inequalities in healthcare. I feel now that I can make a greater difference by working in health policy." Currently, students can choose from one of two tracks within the major: a natural sciences option or a social and behavioral sciences option. Students from both tracks have a foreign language requirement and are encouraged to study abroad their junior year. Both groups also do coursework at the School of Public Health. "Working [alongside] the graduate students is an amazing experience," says Pohl. "They come into the program with so much background. There are physicians, nurses, recent [graduates] of the Peace Corps. It's one of the components of the program I like best." --SD
RETURN TO NOVEMBER 1999 TABLE OF CONTENTS. |