Motor Evoked Potentials
Motor evoked potential (MEPs) are the electromyograph responses of the peripheral muscles to electrical stimulation of the motor cortex. Changes in the MEP signal have been shown to exhibit significant correlation with neurological deficit and spinal cord injury. Analysis of MEP signals can therefore provide a measure of the integrity and functionality of the descending motor pathways of the spinal cord, such as the corticospinal and rubrospinal tracts.
MEPs can be generated in one of two ways:
- Transcranial magnetic stimulation (TMS)
- Direct electrical stimulation
TMS allows for noninvasive stimulation of the motor cortex in a conscious patient. A coil is placed next to the head of the patient, and as electrical current from the coil generates a magnetic field, it produces a current in the motor cortex that triggers peripheral propagation of the stimulus. Direct electrical stimulation requires a craniotomy so that the stimulus can be applied to the cortex. This is more invasive, but is very useful in animal studies in that it allows precise stimulation of specific regions of the cortex.
The MEP signal obtained is the electromyogram generated by the motor action potentials in the peripheral muscle. MEPs are used to test the integrity of the motor pathways. Common clinical applications include assessment and diagnosis of head injuries, paralysis, spine surgery, orthopedic surgery, and others.
Signal Processing
Time vs. Frequency Domain
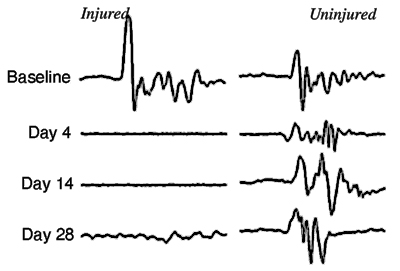
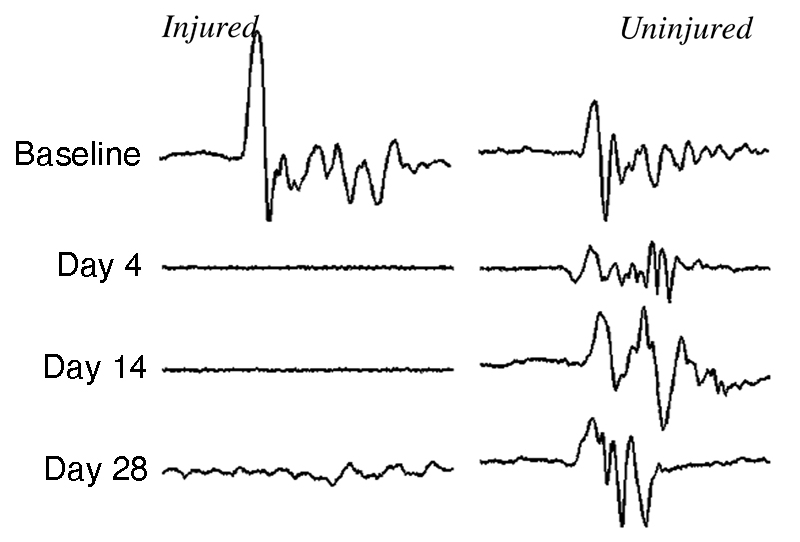
Although time-domain analysis of MEP signals in not normally practiced, in spinal cord injury, the amplitude of the MEP peak is expected to decrease and the latency to increase.
Window Energy Index and Analysis
A window energy index (WEI) is computed from the desired time-frequency window selected from the joint distribution plane to quantify the spinal cord injury changes in the time-frequency plane. The mid-frequency region has been found to be the most sensitive to spinal cord injury related motor evoked potential signal changes during the preliminary rodent studies.
Steps for the window energy index calculation for SCI detection
- Data acquisition and pre-processing
- Time-Frequency analysis
- Comparison and spinal cord injury detection
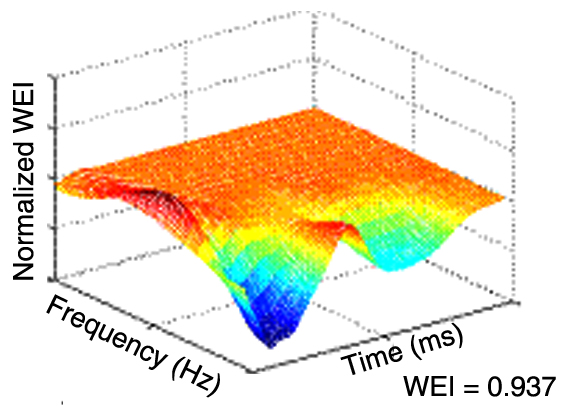
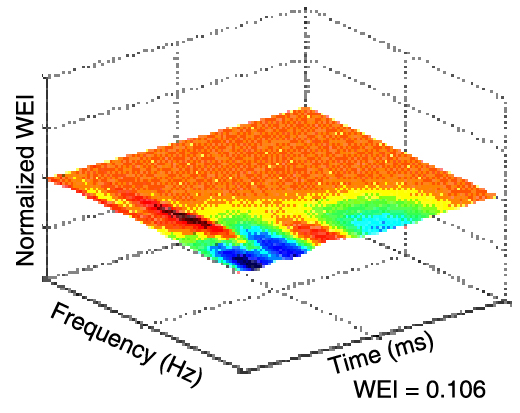
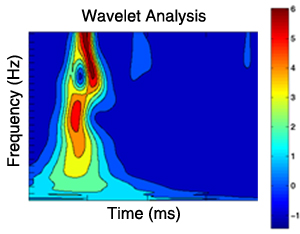
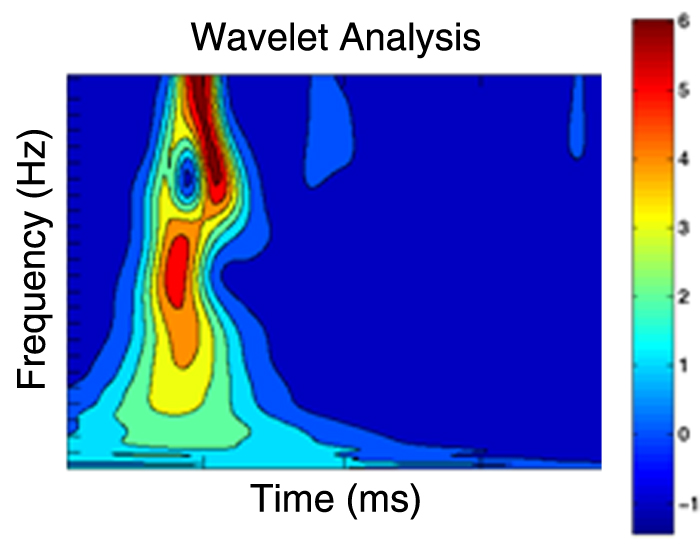
The figures above are 3D illustrations of WEI stimulation using experimental rat data. These show the energy difference of the time-frequency distribution during injury and recovery compared with the MEP baseline signal. Compared to the baselines, the normalized WEI energy change of the injury is 0.937 while the WEI change of recovery is 0.106. The 3D energy distributions in time-frequency domain are capable of accurately capturing and characterizing the spinal cord injury process and even the transition from injury to recovery.
- Faith A. Bazley, Charles Hu, Anil Maybhate, Amir Pourmorteza, Nikta Pashai, Nitish V. Thakor, Candace Kerr, Angelo H. All. "Electrophysiologal evaluation of sensory and motor pathways after incomplete unilateral spinal cord contusion." Submitted to Journal of Neurosurgery: Spine.