STAFF CONTACT INFORMATION
Budget-Capital
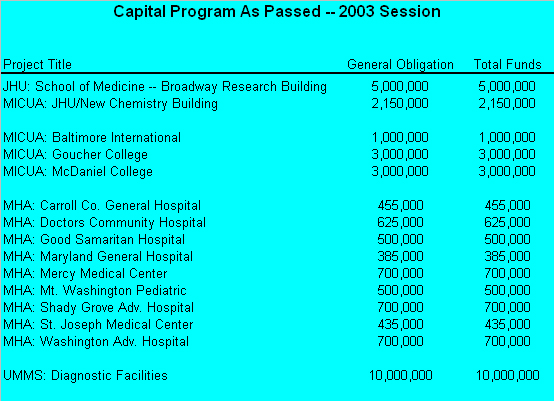
The General Assembly passed a capital budget totaling $2.4 billion including $1.4 billion for the transportation program. Of the total, $740 million is funded with general obligation bonds; about $1.3 billion is funded through pay-as-you-go (PAYGO) funding in the operating budget; and $406 million is funded with revenue bonds, including higher education academic bonds ($33 million) and transportation bonds ($370 million). This year, Johns Hopkins received $7.15 million in the capital budget for two projects that are detailed below. The Maryland Association of Independent Colleges and Universities Association (MICUA) received a total of $7 million for three projects and the Maryland Hospital Association (MHA) received $5 million for 9 capital projects, all of which are listed below.
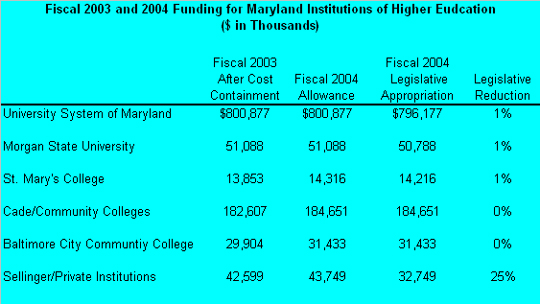
The chart below demonstrates FY 2003 and FY 2004 funding for MD institutions of higher education
School of Medicine--Broadway Research Building ($5 million) - A grant will be provided for construction to assist with the design, construction, and capital equipping of the New Broadway Research Building. Following is a short description:
� 195,000 NASF (379,385 GSF) 10-story facility, on the southeast corner of Broadway and Madison Street, will include laboratories, support facilities, offices, and a core vivarium
� Programs to be housed in the Broadway Research Building include
o Institute for Cell Engineering
o McKusick-Nathans Center for Medical Genetics
o Institute of Molecular Cardiobiology
o Basic and Applied Immunology of Cancer
o Genomics
o Bioinformatics
o DNA Array and Sequencing
o Neurological Oncology/Neuroscience
o Chemistry and Pharmacology
New Chemistry Building ($2.15 million) - The new chemistry building to be situated on the Homewood Campus, will house the active research programs of six organic chemists currently on the faculty, and provide space for three new faculty -- one additional senior faculty member in organic chemistry and two new junior faculty members. It will also provide selected undergraduate and graduate students with additional laboratory space for collaborative research with faculty. The new three-story building will provide approximately 54,000 gross square feet (GSF) of up-to-date replacement research/teaching space, and three additional chemistry laboratories. It will also provide space for a nuclear magnetic resonance (NMR) facility located underground, an ideal location for a powerful magnet spectrometer. A mechanical penthouse is included in the project, as is a new consolidated loading dock to serve the needs of the new NMR facility, the rest of the new building, and other programs of the School.
[ Go to top]
Budget-Operating
The State of Maryland provides essential funding to Johns Hopkins, including critical operating funds for the University's academic divisions under the Sellinger Program of Aid to the Independent Colleges and Universities, funding through the Cigarette Restitution Fund for cancer research and public health initiatives, as well as various programs to support health care access for Maryland citizens. A top priority for Johns Hopkins each year is to ensure that the integrity of these programs remain intact in the State's operating budget.
This year the budget dominated the 2003 Session of the Maryland General Assembly, as the State faced a $400 million deficit in the current fiscal year (FY 2003) and a projected FY 2004 shortfall of $1.2 billion. The new administration proposed to balance the budget through reductions and one time transfers. Additionally, new revenues of nearly $400 million were proposed in conjunction with legislation to permit slot machines at four racing facilities. Subsequent defeat of the administration's slot machine plan and declining revenue projections forced the legislature to make significant reductions to the administration's budget as introduced.
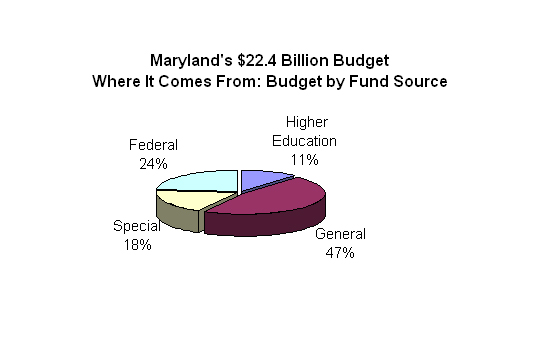
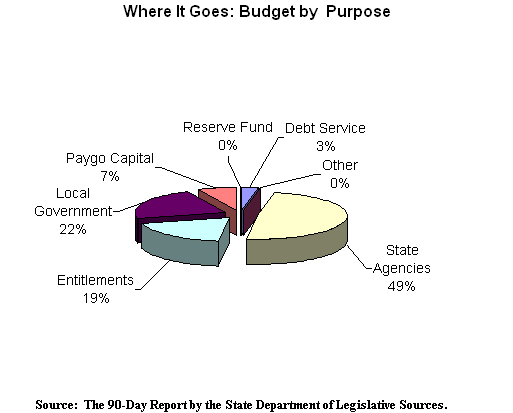
The budget passed by the legislature provides $22.4 billion in appropriations for FY 2004, an increase of $18.5 million (0.1%) over FY 2003. The chart below indicates the funding type by revenue.
For FY 2005, a $688 million deficit is projected. By FY 2008, the gap could be as great as $1.8 billion. The most significant factor driving the out-year fiscal deficits is the cost of implementing the Bridge to Excellence in Public Schools Act. Additionally, the FY 2004 budget was passed contingent on the passage of a tax bill that would address tax compliance measures and subject HMOs and Medicaid MCOs to the 2% premium tax. This bill is expected to raise $135 million in new revenues. The Ehrlich Administration has promised to veto the tax legislation, which will put the FY 2004 budget in a structural imbalance. In order to balance the budget, the Administration has vowed to enact a series of additional cuts to the FY 2004 operating budget.
Should this occur, Johns Hopkins could be severly impacted in several areas, most notable through the Sellinger Aid program and the funding of Medicaid.
Below is a brief summary of other provisions of the FY 2004 budget of interest to Johns
Hopkins:
Cigarette Restitution Fund
� The Governor allocated $4.59 million in FY2004 for the Johns Hopkins Institutions Cigarette Restitution Fund programs that include a cancer research grant and a public health grant to provide a prostate cancer education, screening, prevention and treatment initiative in Baltimore City. Although the Senate proposed a $2 million cut to the cancer research grant, funding was restored during Conference Committee deliberations. Consequently, funding for the Johns Hopkins CRF programs will be at approximately the same level as the FY2003 appropriation.
Higher Education
� Each year, Johns Hopkins receives operating funds that go to the University's Academic Divisions, under the Sellinger Aid program of Aid to Independent Colleges and Universities. This year was challenging for the Sellinger Aid program. In an effort to balance the FY 2004 budget, the Department of Legislative Services recommended limiting the amount of Sellinger funds for institutions based on the number of in-state residents that an institution enrolls. Further, the Department recommended permanently capping the Sellinger program by rebasing the formula at 14.3% per full time equivalent student. If this formula were modified, it would have cut the Sellinger program in half. Efforts by Johns Hopkins and other MICUA institutions prevented the legislature from accepting the Department's recommendations. However, the Legislature did make a one-time reduction of $11 million or 25% to the Sellinger Aid program.
� By comparison, the legislature took no action to reduce FY 2004 appropriations for the Senator John A. Cade formula for community colleges and the Legislature reduced State support for the University System of Maryland by only 0.6%.
Mental Health
� $2 million of the appropriation was restricted until a plan is submitted outlining how the State will operate a network of psychiatric facilities that closes one of the three large regional hospitals, while maintaining existing bed capacity.
� The Mental Hygiene Administration may enter into a privatization agreement for the operation of all or parts of its current facilities. All agreements must be submitted to the budget committee for a 30-day review.
Developmental Disabilities
� By November 15, 2003, DHMH is to report on its plan to close one of the State's residential centers for the developmentally disabled by FY 2005. The report will include how residents will be served either in other state facilities or community settings.
Substance Abuse
� DHMH may not award Baltimore City funding under the Substance Abuse Treatment Outcomes program in FY 2004 to allow other jurisdictions to receive funding.
� DHMH must report by October 1, 2003, on the five-year historical substance abuse funding by jurisdiction to include treatment, prevention, and total number of individuals served. The report will include the estimated need for treatment and criteria for future substance treatment funding by jurisdiction.
� The Department of Veterans Affairs and DHMH must report to the budget committee by October 1, 2003, on the availability of drug treatment for veterans. The report is to include the number of slots in both publicly and privately funded substance abuse treatment programs and the projected need for treatment.
Medicaid and CHIP
� While approving a $3.5 billion total fund appropriation for the program, the budget committee reduced General Funds support for Medicaid program by:
- $3.0 million for MCO capitation rates
- $5.3 million for nursing home reimbursements
- $1.8 million for the Expansion of Waiver for Older Adults
- $3.8 million for the Children Health Program (this reduction is the result of a freezing enrollment in the Children Health Program for families above 200% of the federal poverty level) and requiring a family contribution of 2% for families with income from 185% to 200% of the federal poverty level
- $1.2 million of the MCO Performance Incentive Fund restricted for Medbank
- Added language requiring pharmacy co-payments to be extended to MCO enrollees, generating a savings of $700,000
- $7.5 million restricted to increase fees for dental restorative procedures and DHMH is to develop a plan for increasing utilization of dental care services by October 1, 2003
- Elimination of the Children's Health Program's employer sponsored coverage, transferring these children to the MCOs
Workforce Development
� The Governor's Workforce Investment Board (GWIB) must review the State's efforts related to workforce development to seek efficiency savings and report its recommendations by September 1, 2003.
University of Maryland Medical System
� In FY 2004, the State appropriated $9.7 million to support operations at Montebello at Kernan ($2.7 million) and the Shock Trauma Center ($7.0 million - $3.5 million in operating support and $3.5 million in equipment and technology upgrades).
HB0753
Taxes and Revenues
This bill creates additional revenues totaling $135 million through changes to State corporate income taxation; a 10% corporate income tax surcharge for tax years 2003, 2004, and 2005; and a two percent insurance premium tax on health maintenance organizations and medicaid managed care organizations. These dollars were a crucial
component in balancing the fiscal 2004 budget.
Of specific interest to Johns Hopkins is the two percent insurance premium tax on Health Maintenance Organizations and Medicaid Managed Care Organizations. The bill imposes the two percent insurance premium tax on Health Maintenance Organizations (HMO's) and Managed Care Organizations (MCO's) that is currently imposed on all gross direct insurance premiums derived from businesses in Maryland. All health insurers, other than nonprofit health service plans, fraternal benefit societies, and HMO's currently are subject to the premium tax. Although an MCO is not considered an insurer, the gross receipts received by an MCO as a result of capitation payments by the Department of Health and Mental Hygiene will be subject to the premium tax. Applying the two percent premium tax to these organizations will raise at least $48.9 million in fiscal 2004.
Effective Date: July 1, 2003
For more information, please contact:
Bret Schreiber
HB0935
Budget Reconciliation and Financing Act of 2003
The Budget Reconciliation and Financing Act (BRFA) of 2003 (House Bill 935) is an integral component of the plan to balance the State's operating budget in FY 2003 and 2004. The Act institutes a number of one-time transfers from various funds to the general fund. Almost $416 million will be transferred in FY 2003 and over $329 million will be transferred in FY 2004.
The Act includes various provisions that increase FY 2004 general fund revenues by $163 million and special fund revenues by $19.3 million. Also, several actions related to tax compliance measures generate $43.3 million in general fund revenue. Other revenue-generating actions eliminate the graduated withholding (one-time only), cap the Heritage Tax Credit, and increases fees for land records, medical vital records and vehicle identification cards.
Of interest to Johns Hopkins are provisions in this bill that require Maryland income tax withheld by an employer to be remitted within three business days after payroll (which, for most employers is biweekly), when $700 of liability is reached, and if total withholding for the prior calendar year was $15,000 or more. This provision takes effect
January 1, 2004. Because $15,000 of withholding for a calendar year equates to approximately $250,000 of wages, most businesses will be required to withhold more frequently than under current law.
Additionally, the bill requires that before various licenses or permits may be renewed, the issuing authority must verify through the Comptrollers office that the applicant has paid all undisputed taxes and unemployment insurance contributions, or that the applicant has provided for payment in another manner. Covered licenses and
permits include those governing business and occupations and professions, health occupations and other types of licenses and permits.
The Act also requires families participating in the Maryland Children's Health Program who have incomes between 185 and 200% of the federal poverty guidelines (FPG) to pay a premium. The Act also eliminates the employer sponsored coverage component of the Maryland Children's Health Program.
Also of interest to Johns Hopkins are provisions which impact the Maryland Heritage Structure Rehabilitation Tax Credit. Originally, House Bill 341 was introduced which would have eliminated the Maryland Heritage Structure Rehabilitation Tax Credit. However, the General Assembly voted to the Program, which has provided support to Johns Hopkins projects at the Peabody Institute, Eastern High School and other projects on the East Baltimore Campus. The conference committee reached a compromise by establishing an aggregate cap on tax credits for commercial projects while leaving the credit for homeowners unchanged. Additionally, the following amendments were agreed upon and included in the Budget Reconciliation and Financing Act.
1) $23 million cap on credits for commercial properties for the period from February 1 through December 31, 2003,
2) $15 million cap on credits for commercial properties for calendar year 2004 (with the June 1, 2004 sunset),
3) the cap applies to Part II approvals that will be given on a first-come, first-served basis, and
4) the existing sunset date of June 1, 2004 for the entire program remains in place.
Finally, the BRFA reduces the amount of Sellinger Funds we receive from the State of Maryland by 3.1% in FY 2003. This reduction will also impact our FY 2004 funding level. The 3.1% reduction equates to about $543,000 for Johns Hopkins University.
For more information, please contact:
Bret Schreiber
[ Go to top]
Economic Development
Much of the attention this Session focused on the budget and the State's fiscal challenges. Policy initiatives whose enactment would have required the use of new State operating funds to implement were rejected. As a result, policy initiatives focusing on the economic development needs of Maryland were limited in numbers. Several pieces of legislation were not passed into law such as allowing portions of the State's pension funds to be invested in biotechnology parks, and the creation of a commission to study the State's procurement initiatives.
Baltimore City and Johns Hopkins Communities: Issues of importance to Baltimore City and
to the communities surrounding Johns Hopkins' campuses included such topics as condemnation
of distressed property, community association liability and funding for neighborhood intervention projects through the Community Legacy Program.
Following are the legislative priorities of Johns Hopkins for economic development, including bills specific to Baltimore City and communities, that were enacted this year.
HB0424
Baltimore City - Condemnation - Immediate Possession and Title - Distressed Property
This bill authorized proceedings for condemnation and immediate taking of distressed properties in Baltimore City. The bill also granted exclusive original civil jurisdiction of a specified proceeding to the District Court.
Effective Date: October 1, 2003
For more information, please contact:
Bret Schreiber
HB0467
Community Associations - Civil Liability
This bill limited the civil liability of community associations and their agents by including them under the Maryland Associations, Organizations, and Agents Act, through which they may register with the Secretary of State.
Effective Date: October 1, 2003
For more information, please contact:
Bret Schreiber
HB0620
Housing - Community Legacy Program - Neighborhood Intervention Projects
This bill redefined a neighborhood intervention project as a project sponsored by a Community Development Financial Institution (CDFI). It would assist owner-occupants, community development organizations, or local governments, to buy and redevelop property that needs rehabilitation and is located in an otherwise stable neighborhood. CDFIs may sponsor community legacy projects and the Community Legacy Board should give priority to project applications that provide for likely repayment of the financial assistance to a CDFI, or to the Community Legacy Financial Assistance Fund (CLFAF). The Board could also waive the requirements for a community legacy area designation and a community legacy plan for neighborhood intervention projects. Financial assistance awards under a community legacy agreement can be no greater than $500,000, and the board is required to allocate at least 15% of the CLFAF to the neighborhood intervention projects.
Effective Date: July 1, 2003.
For more information, please contact:
Bret Schreiber
HB1152
Baltimore City - Charles Village Community Benefits District - Continuation of Authority
This bill modified the Charter of Baltimore City by requiring the Mayor and City Council to review and decide on the continuation of each community benefits district every four years beginning with the 1st meeting in December 2001 (therefore applied retroactively) for the Charles Village Community Benefits District. It also declared the intent of the General Assembly that the Charles Village Community Benefits District has been continuous since June 1, 1994, and will remain, unless the Mayor and City Council of Baltimore terminate it.
Since the Homewood campus of Johns Hopkins borders on the Charles Village Community Benefits District, we monitored the progress of this legislation on their behalf, and kept its leadership up to date on its progress as it moved through the legislature.
Effective Date: June 1, 2003
For more information, please contact:
Bret Schreiber
[ Go to top]
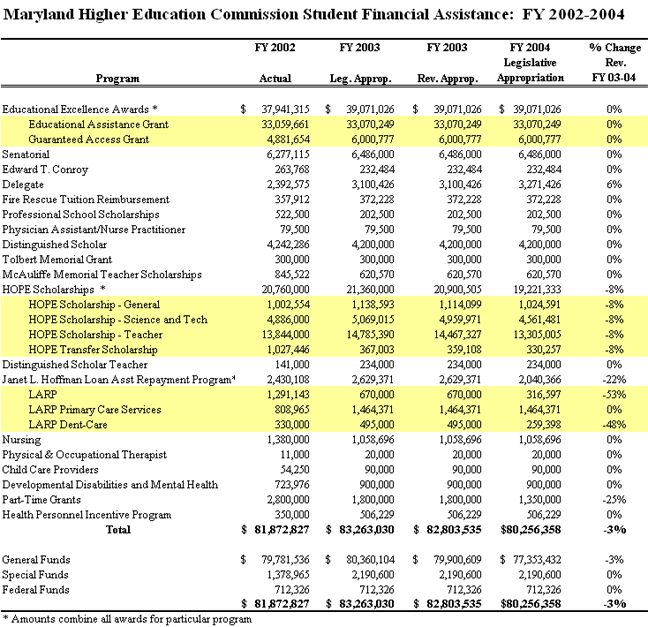
Financial Aid and
Scholarships
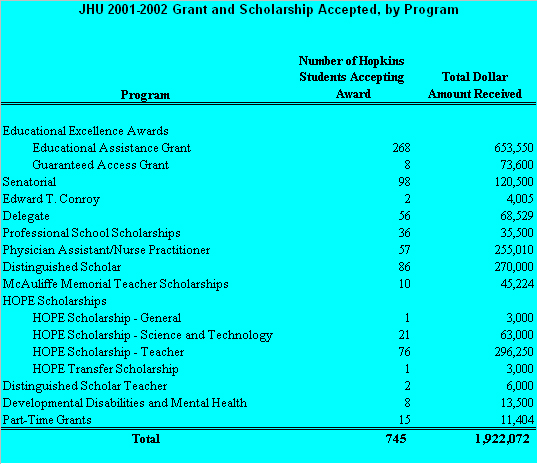
The total FY 2004 appropriation for State financial aid is $80.2 million, a 3% decrease from FY 2003. Of that total, 48% is allocated for need-based financial aid ($39.1 million) and 24% is allocated for the HOPE Scholarship Programs ($19.2 million). Another 27% includes several workforce shortage and merit-based financial aid programs. On average, most State scholarship programs retained the same funding levels as in FY 2003. However, the HOPE Scholarship programs, which include General, Science and Technology, Teacher and Transfer Scholarship awards, were reduced by 8% from the FY 2003 appropriation.
Students attending Johns Hopkins significantly benefit from many State Scholarship Programs. For the 2002-2003 academic year, Johns Hopkins students received a total of $1.9 million in grants and scholarships from the State of Maryland, an increase of 4% over last year. The charts below demonstrate the total amount of State dollars appropriated in FY 2004 for the State Scholarship Programs. The next chart demonstrates the total number of Johns Hopkins students who received State grants and scholarships, and the total dollars for each grant and scholarship program in FY 2003.
HB0774
Higher Education - Educational Excellence Awards - Funding
House Bill 774/Senate Bill 568 addresses the decentralization of funding for the Educational Excellence Awards program (EEA). The College Readiness for Disadvantaged and Capable Students Act of 2002 provided for the decentralization of a portion of the EEA, if State funding was available. These bills will require the Maryland
Higher Education Commission to transfer at least $2 million from the scholarship funds that are unspent and retained by the commission each year to Maryland institutions of higher education. The institutions, rather than the Office of Student Financial Assistance, will be allowed to use the funds to provide the EEA to students who meet the requirements of the award, but apply after the deadline or have other extenuating
circumstances. Our colleagues at MICUA helped to ensure that the funds used were unspent or unused funds, rather than monies that would be taken directly from the existing funds that our utilized by Johns Hopkins and the other MICUA institutions. Johns Hopkins students receive over $600,000 each year in EEA grants.
Effective Date: October 1, 2003
For more information, please contact:
Bret Schreiber
[ Go to top]
General Education
The primary focus in education this year was budgetary support to help pay the first year of the phase-in scheduled for the new education finance structure established by the Bridge to Excellence In Public Schools Act of 2002 (recommendations from the Thorton Commission). Full funding for the first year of the program ($238 million) was included in the Governor's proposed FY 2004 budget, however the General Assembly reduced that amount to $206 million. Even with the General Assembly's reductions, the final appropriation for FY 2004 for public education represents a 6.6% increase from FY 2003 and preserves the integrity of the financing structure. While the State's remarkably difficult fiscal situation made additional policy initiatives difficult to pass, the following bills were legislative priorities for our primary and secondary education programs.
SB295 would have established a program of salary grants with the goal of improving recruitment and retention of well-qualified principals, vice-principals and assistant principals. This legislation supported the recommendations of the Maryland Task Force on the Principalship and the Visionary Panel's Leadership Task Group, which recognized the great need for highly skilled principals who understand and support Maryland's school reform agenda. SB295 would have helped implement reforms, but the costs associated with implementation proved too great during a time of fiscal crisis in Maryland, and the bill failed.
SB0075
Public Charter School Act of 2003
This bill establishes a Maryland Public Charter School Program with primary chartering authority granted to local boards of education. Secondary chartering authority is granted to the Maryland State Board of Education (MSDE) in its capacity to review appeals of a local board's decision to deny a charter or as the chartering authority for a restructured school. This bill allows the public school staff, parents or guardians of public school students, nonsectarian nonprofit entities, or nonsectarian institutions of higher education in the State to apply to establish a public charter school. The bill requires the professional staff members of a public charter school to hold the
appropriate Maryland certification. This bill also requires the MSDE to establish and distribute to local boards of education model public charter school policy language that can be used to create local public charter school policies. The establishment of public charter schools was a top priority of the Ehrlich Administration and will allow the awarding of federal funds to go to
Maryland to help organize public charter schools.
Effective Date: July 1, 2003
For more information, please contact:
Bret Schreiber
[ Go to top]
General Health Care
Each year there are numerous bills introduced that impact the entire health care delivery system. This year, several bills were introduced that proposed to create new commissions and advisory boards, such as creating the Maryland Home Care Services Commission, which failed to gain final approval. Other bills attempted to create additional funding sources to support efforts such as breast cancer research. Due to the State's budget crisis, these efforts also generally failed. One bill that did pass could impact all aspects of Maryland health care delivery system. A task force will be created to examine how to restructure the Maryland Department of Health and Mental Hygiene. With the fiscal crisis, this reorganization may produce budgetary savings for the state, and may affect health care providers efforts to provide care.
HB0272
Vital Statistics-Certificate of Birth Resulting in Stillbirth
This bill requires the Secretary of the Department of Health and Mental Hygiene to make available a certificate of birth resulting in stillbirth to the parent of a stillborn child. The birth is still registered with vital statistics as a fetal death. The Department is responsible for implementing the process for issuing the certificates, and fulfilling the requests for a
certificate of stillbirth to any parent that received a certificate of fetal death prior to the
enactment of the legislation. The parents may choose whether the child's first name should appear on the certificate or not. The Department must report to the General Assembly on the status of the program by October 1, 2005.
Effective Date: June 1, 2003
Signed by the Governor on April 22, 2003; Chapter #136
For more information, please contact:
Sheila Higdon
HB0465
Baltimore City Health Department - Designation of Nonprofit and Quasi-Governmental Entities - Alcohol and Drug Abuse Administration Funds
This Act allows the Baltimore City Health Department to designate a nonprofit or
quasi-governmental entity in Baltimore City to receive funds from the Alcohol and Drug Abuse Administration to plan, manage, monitor, and disburse funds to substance abuse prevention and treatment programs. The City Health Department may revoke an entity's designation at any time except to the extent that the Administration, the designee, or both have acted in reliance of the designation. The Administration will have a direct relationship with the designee (having the same rights and remedies as it would have with the Baltimore City Health Department) and will disburse the funds directly to the designee.
Effective Date: October 1, 2003
For more information, please contact:
Nicole Xander
HB0478
Money Follows the Individual Fund
This bill prohibits DHMH from denying an individual access to a home- and community-based services waiver due to a lack of funding for waiver services if:
1) the individual is living in a nursing home at the time of the application for waiver services,
2) the nursing home services for the individual were paid by the program for at least 30 consecutive days immediately prior to the application, and
3) the individual meets all of the eligibility criteria for a participating home and
community-based services provided to the individual would quality for Federal matching
funds.
By September 1, 2003, the Department of Health is required to notify all nursing home residents whose nursing home services were paid for by the Maryland Medical Assistance Program about the opportunity to apply for home - and community-based services.
By January 1, of each year, the Secretary is required to submit a report to the General
Assembly on efforts to promote home - and community-based services under this Act and the number of individuals who have transitioned from nursing homes to home-and community-based waiver services.
Effective Date: July 1, 2003
For more information, please contact:
Sheila Higdon
HB0761
Task Force to Study the Reorganization of the Department of Health and Mental Hygiene
The act establishes the Task Force to Study the Reorganization of the Department of Health and Mental Hygiene (DHMH). The primary objective of the Task Force is to study ways to improve the delivery of health and mental health services in Maryland. Included in this mandate are calls for specific studies on the structure of DHMH, the
impact of removing the Developmental Disabilities Administration, the Mental Hygiene
Administration and the Maryland Medical Assistance Program from the Department, and the organization of health departments in other states.
The act establishes a Task Force of 26 members comprised from the following organizations:
1) Two members from the Senate of Maryland,
2) Two members from the House of Delegates,
3) Three representatives from the DHMH,
4) One representative from the Department of Budget and Management),
5) One local health officer appointed by the DHMH,
6) One representative from the Association of Maryland Hospitals and Health Systems,
7) One representative from the Mental Health Association of Maryland,
8) One representative from the Maryland Association of Nonprofit Organizations,
9) One individual with expertise in reorganization of State agencies,
10) The Special Secretary for Children, Youth, and Families, or the Special Secretary's
designee,
11) One representative from the Office of Individuals with Disabilities,
12) One representative from the American Federation of State, County and Municipal Employees,
13) One representative from the Medical and Chirurgical Faculty of Maryland,
14) One representative from the State's public academic health center,
15) One representative from Mid-Atlantic LifeSpan,
16) One representative from the Maryland Nurses Association,
17) One representative from the Health Facilities Association of Maryland,
18) One representative from the Advocates for Children and Youth,
19) One representative from the Maryland Association of Adult Day Services, and
20) One representative from a HealthChoice managed care organization, appointed by the Department of Health and Mental Hygiene.
The Task Force is required to report its findings to the Governor and the General Assembly on or before December
1, 2004.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
SB0031
Informal Kinship Care - Consent to Health Care on Behalf of a Child
The section allows a relative who is providing kinship care for a child to consent to health care services on behalf of the child, if the court has not appointed a guardian, and the relative verifies the kinship care through a sworn affidavit. The affidavit is required to include information such as name and age of the child, nature of serious family hardship that has lead to the kinship care, and the relationship between the child and relative providing care.
Affidavit forms are required to be available at the local department of education and
department of health. The affidavit must be filed annually with the local department of social services. The relative is to notify the department within 30 days of any changes in the care of the child, serious family hardship, or relative providing care. A copy of the affidavit shall be provided to the health care provider treating the child.
Effective Date: October 1, 2003
For more information, please contact:
Jim Kaufman
[ Go to top]
Health Care Facilities
Again this year, the General Assembly considered numerous pieces of legislation to alter or abolish the Certificate of Need process. Several bills were introduced, and defeated that would have: 1) eliminated open heart CON and required licensure or 2) required the Health Care Commission to granted a CON to hospitals participating in the C-PORT program. This year, most of the discussion surrounding CON focused on a proposed amendment that would have decoupled angioplasty and on site open heart surgery backup. However, the amendment was not accepted since the Maryland Health Care Commission is currently addressing this issue and is planning a research study to examine the safety and efficacy of decoupling these services.
In addition, the General Assembly adopted several bills that will impact how health care
facilities deliver care. SB 732 - Hospice Care Prohibition (see summary below) prohibits the Health Care Commission from granting a person the authority to operate a statewide CON, while SB 479 - Trauma System Funding Act (see summary below) will provide resources to the State's trauma system.
Legislation was also introduced again this year regarding the use of cameras in nursing homes. One bill, known as Vera's Law, passed and requires the Department of Health to develop guidelines for a nursing home that elects to use electronic monitoring with the consent of the resident. Another bill that would have required installation of cameras failed.
HB0553
Nursing Homes - Third Party Liability Reviews and Audits
The Act requires a nursing home that receives payment from the medical assistance program to provide a report of the credit balances of the nursing home to the Department of Health and Mental Hygiene (DHMH) on a quarterly basis, and DHMH shall conduct a third party liability review of the report. In addition, DHMH may conduct a third party liability audit of a random sample of the reports of credit balances. DHMH may also conduct a third party liability audit of a nursing home that is found to be noncompliant as a result of the audit of a random sample of reports of credit balances. DHMH will be required to establish a process by which nursing homes may appeal the results of a third party liability audit.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
HB0780
Emergency Telephone System - Wireless Enhanced 911 Service
House Bill 780 and Senate Bill 549 requires the implementation of wireless enhanced 911 service. It adds two members to the Emergency Number Systems Board and specifies county representation on the board. The language requires each subscriber to pay a 911 fee with each phone bill. Individual lines would not be subject to the fee. The fee is 25 cents per month and the county imposed fee limit was increased to 75 cents per month.
The fee increase should not significantly impact the charges to Centrex or PBX phone systems.
Effective Date: October 1, 2003
For more information, please contact:
Jim Kaufman
HB0884
Work, Not Welfare, and Qualifying Employees with Disabilities Tax Credits
This bill extends the sunset provision for the Employment Opportunity Credit, a tax credit to employers that hire qualified employment opportunity employees or qualifying individuals with disabilities, to June 30, 2006. Credits may be carried forward for tax years beginning after January 1, 2009. The credit applies to companies that pay state income taxes, financial institution franchise taxes, public service company franchise taxes, and non-profit tax-exempt organizations that have unrelated business income that is taxable for wages and child care expenses paid to qualified employees.
Effective Date: July 1, 2003
For more information, please contact:
Jim Kaufman
HB1065
Health Services Cost Review Commission - Appointment of Members
The section states that the Governor shall give consideration to and make appointments when
appropriate that would promote racial, gender, and geographic diversity on the Health Services
Cost Review Commission.
Effective Date: October 1, 2003
For more information, please contact:
Jim Kaufman
SB0284
Public Records - Motor Vehicle Records - Access by Hospitals
This bill amends the current statute governing the dissemination of personal information relating to the ownership of vehicles. This action would allow hospitals to acquire the personal information on the owner of any vehicle parked on hospital property. The information can be used for security purposes only.
Effective Date: October 1, 2003
Signed by the Governor on April 8, 2003; Chapter #19
For more information, please contact:
Nicole Xander
SB0303
Division of Labor and Industry and Associated Boards and Councils - Sunset Extension and Program Evaluation
SB303/HB651 extends the termination dates of various boards, councils, and services. Most importantly, it lifts the licensure requirements for employment agencies and changes the definition of "home health agency" to any nurse registry that is an employment agency under the Maryland Employment Agency Act. Employment Agencies will still be required to pay advance fees and must be bonded, and home care agencies will still be required to meet quality standards.
Effective Date: July 1, 2003
For more information, please contact:
Nicole Xander
SB0479
Maryland Trauma System Funding Act
The act establishes the Maryland Trauma Physician Services Fund, which will be supported by a $2.50 surcharge on automobile registrations. The fund, will be administered by the Maryland Health Care Commission (MHCC) and the Maryland Health Services Cost Review Commission (HSCRC).
The purpose of the fund is to subsidize the documented costs of physician care provided to trauma patients, reported on the trauma registry, cared for in a designated adult and pediatric trauma centers. The fund will provide subsidies for physician uncompensated care and to increase low Medicaid reimbursement rates, up to
100% of comparable Medicare rates. In addition, the fund will be used to provide support for trauma center on-call costs. The methodology shall reimburse on-call costs at a rate based upon the reasonable costs equivalents for the specialty using the physician compensation components of the Medicare economic index. For Level III trauma centers, the subsidy will equal 30% of the rate, while the subsidy for Level II centers will equal 20% of the rate.
Proceeds from the fund will be distributed based on a methodology established jointly by the MHCC and the HSCRC. The allocation methodology is to take into account:
1) Amount of physician uncompensated care,
2) Amount of under compensated care attributable to Medicaid,
3) Costs of maintaining trauma physician on-call,
4) Number of Maryland patients served by a trauma physician,
5) Extent to which trauma costs are subsidized by the hospital or other sources, and
6) Extent to which trauma costs are not covered by hospital rates.
Before September 1, of each year, MHCC and the HSCRC are required to report to the General Assembly on the amount of money in the fund, the amount of money distributed to physicians and trauma centers, recommendations on altering the manner in which trauma physician uncompensated care costs are reimbursed, and the amount that each hospital contributed towards the subsidization of trauma related costs
The act also creates an eight-member legislative committee to study and make recommendations on the structure and funding the State's emergency medical response system. This committee is to provide an interim report by December 31, 2003 and a final report by December 1, 2004, and shall review the following:
1) Current and projected fund balanced of MEMSOF and the funds usage,
2) Long-term operating and capital needs of the trauma centers,
3) Funding needs of fire responders and emergency medical personnel,
4) Incentives for illness and injury prevention,
5) Funding mechanisms to meet the needs of the emergency medical system,
6) Availability of federal homeland security funding,
7) Oversight and accountability of MEMSOF,
8) Current use of State Police helicopters and the potential use of private helicopter
companies,
9) Licensing of commercial air ambulances,
10) Plans to finance the replacement of the State Police's helicopters,
11) The purpose and use of funds previously appropriated from MEMSOF, and
12) Structure and function of MIEMSS.
The act also requires MIEMSS to study whether the need exists to enter into an agreement with an adult trauma center located in Washington D.C. to ensure access to care for Maryland patients. The study is to consider duplication of services and the centers ability to sustain necessary patient volumes.
The HSCRC is also required to report to the General Assembly by September 1, 2003, and December 31, 2003, on the anticipated time frame in which trauma stand-by costs will be included in hospital rates and the regulatory costs of providing trauma care that may not be included in hospital rates.
Effective Date: July 1, 2003 (Sunset December 31, 2004)
For more information, please contact:
Jim Kaufman
SB0549
Emergency Telephone System-Wireless Enhanced 911 Service
This bill implements a plan for wireless enhanced 911 service. It adds two members to the Emergency Number Systems Board and specifies county representation on the board. The language requires each subscriber to pay a 911 fee with each phone bill. Individual lines would not be subject to the fee. The fee is 25 cents per month and the county imposed fee limit was increased to 75 cents per month. The fee increase should not significantly impact the charges to Centrex or PBX phone systems.
Effective Date: October 1, 2003
For more information, please contact:
Jim Kaufman
SB0732
Maryland Health Care Commission - Hospice Care - Prohibition
The act amends the existing CON statute regarding general hospice care programs. Under the amendment, the purchaser of a general hospice care CON may only acquire the authority to provide home-based hospice services in the same jurisdiction in which the seller of the CON provided home-based hospice services as of December 31, 2001. However, a general hospice may provide home-based services for patients upon immediate discharge from a health care facility/system, regardless of jurisdiction, if the hospice is either a hospital based hospice or had an agreement with the health care facility/system before April 5, 2003.
Language was also added to clarify that the Health Care Commission may not issue a CON or determination on the acquisition of a general hospice care program to provider home-based services on a statewide basis.
The act also requires the Health Care Commission to complete a study, before January 1, 2004, on the status of CONs for hospice services and efforts to update the State Health Plan Hospice Chapter. In updating the State's Health Plan, the Commission may not relay only data collection from nongovernmental sources.
Effective Date: July 1, 2003
For more information, please contact:
Jim Kaufman
[ Go to top]
Health Care
Practitioners
Following failed legislation that would have extended the Board of Physicians Quality Assurance during the 2002 Session, and contentious negotiations down to the final week of the 2003 Session, SB500 was passed that constitutes a new Board of Physicians (see summary below). A major compromise was achieved regarding the evidentiary standard, allowing the clear and convincing standard to remain in effect when assessing the charge of failure to meet the appropriate standard of care.
The Maryland Hospital Association, Johns Hopkins Medicine, the Board of Nursing, and others collaborated to secure passage of HB343 (summary below) that will allow a hospital's designated infectious disease/communicable disease officer to order an HIV test if there has been an exposure between a patient and a health care provider that, in accordance with CDC guidelines, would warrant recommending or offering chemoprophylaxis treatment when informed consent or substitute consent was sought and the patient was unavailable or unable to consent.
HB0164
Health Occupations - Medical Review Committees
This bill expands the category of medical review committees to include the Maryland Patient Safety Center, which was proposed by the Maryland Health Care Commission. This provision will sunset if the Maryland Patient Safety Center is not established by June 30, 2005.
Effective Date: July 1, 2003
Signed by the Governor on April 22, 2004; Chapter #126
For more information, please contact:
Sheila Higdon
HB0310
State Board of Social Work Examiners - Sunset Extension and Program Evaluation
This Act extends the sunset date for State Board of Social Work to July 1, 2014, and requires an evaluation by July 1, 2013. The Act also requires that a licensee of any license level shall be appointed (if qualified) if a licensed social work associate or licensed graduate social worker has not been appointed to the State Board of
Social Work within six months of a vacancy.
Also, by October 2003, the Board and the Department of Health and Mental Hygiene shall report to the General Assembly on the implementation of the recommendations of the Department of Legislative Services contained in the sunset evaluation report dated October 2002.
Effective Date: July 1, 2003
For more information, please contact:
Nicole Xander
HB0343
Hospitals - HIV Testing - Health Care Providers
This chapter would allow the designated infectious disease/communicable disease officer at hospitals to order an HIV test of blood samples already obtained, and blood samples or other body fluids collected for the purpose of HIV testing. The following criteria must be met in order to test:
1) An exposure has occurred between a patient and health care provider or first responder that (in accordance to Centers for Disease Control recommendations) would warrant recommending or offering chemoprophylaxis treatment,
2) Informed consent was sought and the patient or appropriate substitute decision maker was either unavailable or unable to consent,
3) The health care provider involved has given prompt notice of the exposure,
4) The health care provider has given informed consent and has submitted a blood sample for HIV testing, and
5) The designated infectious disease/communicable disease officer has made a determination that the HIV test would be helpful in managing the risk of disease and health outcome of the health care provider.
The designated infectious disease/communicable disease officer shall directly notify the patient of the results, and to the extent possible, in a manner that will protect confidentiality of the health care provider and the patient. If the results are positive appropriate counseling and treatment recommendations shall be provided or arranged
for the provider and the patient.
Any physician's order for an HIV test or the results may not be documented in the medical record of the patient or health care provider. The medical records are confidential, and not discoverable or admissible in any criminal, civil, or administrative action.
Hospitals shall maintain a separate confidential record or incident report for the tests and adopt procedures for confidential testing. Any costs incurred in performing an HIV test shall be paid by the hospital. A health care provider, hospital, or hospital designee acting in good faith to provide notification, or maintain the confidentiality of the results, may not be held liable in any cause of action related to a breach of patient or health care provider confidentiality.
In addition, the AIDS Administration in consultation with the Maryland Hospital Association and IDS advocacy originations are to study the issue of HIV testing of individuals who refuse to consent to HIV testing when there has been an exposure of a health care provider. The AIDS Administration is to report the General Assembly by
December 1, 2003, on its findings and recommendations.
Effective Date: October 1, 2003
Signed by the Governor on April 22, 2003; Chapter # 143
For more information, please contact:
Nicole Xander
HB0883
Health Care Disparities Program - Required Education for Practitioners and Coordination of Services
The bill encourages institutions of higher education in the State to include courses or seminars in their curriculum for heal care professional licensure that address the identification and elimination of health care services disparities. It also encourages hospitals with continuing education programs to offer and require the medical staff and health care practitioners to take CME or CEU courses that address health care services
disparities of minority populations.
The bill requires the Department of Health and Mental Hygiene (DHMH) to develop and implement a plan to reduce health care disparities based on gender, race, ethnicity and poverty in consultation with other organizations, including:
1) Maryland Health Care Foundation,
2) Med Chi,
3) Monumental City Medical Society,
4) Nurse Practitioners Association of Maryland,
5) Maryland Academy of Physician Assistants,
6) Mental Hygiene Administration,
7) Center for Poverty Solutions,
8) Morgan State University Graduate Public Health Program,
9) Johns Hopkins Bloomberg School of Public Health,
10) Mid-Atlantic Association of Community Health Centers,
11) Maryland Higher Education Commission,
12) Maryland Hospital Association,
13) Academic Medical Center,
14) Medical School,
15) Nursing Program that offers a Bachelor's Degree in Nursing,
16) Nursing Program that offers an Associate's Degree in Nursing,
17) Maryland Nurses Association,
18) National Black Nurses Association, and
19) University of Maryland School of Social Work.
The Maryland Health Care Foundation, Morgan State University Graduate Public Health Program, the Johns Hopkins Bloomberg School of Public Health, and the Monumental City Medical Society must provide staffing and other assistance to implement the plan, which must include recommendations to coordinate existing
programs related to health care disparities by:
1) identifying available funding,
2) identifying any gaps in service delivery based on gender, race, ethnicity and poverty,
3) reducing the duplication of available health care services,
4) reducing the fragmentation of health care services, and
5) identifying outcome measures to reduce health care disparities
By September 30, 2004, DHMH and the other entities involved in plan development and implementation must:
1) examine current continuing education programs offered by hospital and physician organizations that focus on health care disparities and examine CME requirements of each health occupations board,
2) determine the content of a model course or seminar that addresses health care services
disparities of minority populations
3) assess the feasibility of requiring health care providers to take specific courses or
seminars, and
4) identify the oversight that would be required by a health occupation board in order to
determine compliance with continuing education requirements concerning health care disparities.
DHMH will be required to submit a report to the Governor and General Assembly by September 30, of each year on the implementation of a coordinated program delivery system. In addition, DHMH, in consultation with the Mental Hygiene Administration, and the Advisory Council on Health Disease and Stroke, must submit a report to the
Senate Education, Health and Environmental Affairs Committee and the House Health and Government Operations Committee by September 30, 2004, on recommendations and implementation plans for closing gaps in health services delivery and financial access to health services based on race, poverty, gender, and ethnicity. The bill's provisions requiring the development and implementation of the plan to reduce health disparities
terminates September 30, 2008.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
SB0224
Board of Physician Quality Assurance - Office-Based, Medication-Assisted Opioid Addiction Therapy
This law requires the State Board of Physician Quality Assurance (BPQA) to establish or designate a program to train physicians who wish to apply for a waiver from the federal Substance Abuse and Mental Health Services Administration (SAMHSA) to practice office based, medication-assisted opioid addiction therapy by November 1,
2003. In doing so, the BPQA shall consult the Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office and adopt regulations regarding experience or training qualifications.
The Board is also required to educate physicians about the federal law (Drug Addiction Treatment Act of 2000) authorizing the practice of office based medication-assisted opioid addiction therapy; encourage family practitioners and primary care providers; and inform physicians about the availability of training and experience to
qualify for a waiver to practice office-based, medication-assisted addiction therapy.
Effective Date: October 1, 2003
For more information, please contact:
Nicole Xander
SB0387
Department of Health and Mental Hygiene-Selling and Dispensing of Contact Lenses and Replacement Contact Lenses
This act clarifies current statute regarding the writing and dispensing of replacement contact lens prescriptions. The act requires the Department of Health and Mental Hygiene to adopt regulations concerning the sale and prescription of Plano and Zero Powered Contact Lenses and replacement contact lenses. The act includes a section that explicitly identifies the sale or dispensing of contacts without a prescription as a
misdemeanor, subject to a $1,000 fine.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
SB0500
Department of Health and Mental Hygiene - State Board of Physicians
This bill renames the State Board of Physician Quality Assurance (BPQA) to the State Board of Physicians (Board), and increases Board membership from 15 to 21. The new Board will be appointed by the Governor with the advice of the Secretary of Health, and the advice and consent of the Senate, by August 1, 2003. Membership
will include:
1) 11 practicing licensed physicians,
2) 1 of whom shall be a Doctor of Osteopathy,
3) 1 appointed at the Governor's discretion,
4) 1 representing DHMH,
5) 1 who practices complementary and alternative methods of care,
6) 1 physician will hold a fulltime faculty appointment and will be a representative of academic medical institutions, appointed from a list containing three names from the Johns Hopkins University School of Medicine, and three names from the University of Maryland, and
7) 5 consumer members will be appointed with the advice and consent of the Senate; including a public member knowledgeable in risk management or quality assurance matters appointed from a list submitted by the Maryland Hospital Association (MHA). The consumer member may not have a substantial personal, business, professional or pecuniary connection with a medical field or with an institution of medical education or a health care facility.
The Chairman of the Board will not be appointed by the Governor, but will be elected by the Board members. The bill also stipulates how physicians will be notified of a vacancy on the Board and prohibits reappointment, or appointment of a physician from a particular medical specialty, if there are two current members serving on the
Board from the same medical specialty.
The Board of Physicians Fund may set reasonable fees for the issuance and renewal of licenses and its other services; fees are to be set at the approximate cost of maintaining the Board. In addition, the Board shall fund the budget of the Physician Rehabilitation Committee (PRC), that is responsible for evaluating and providing assistance to impaired physicians in need of treatment and rehabilitation for alcoholism, chemical dependency
or other physical, emotional or mental conditions. The Medical Chirurgical Faculty of the State of Maryland (MEDCHI) shall appoint the members of the PRC and the Chairman of the Board shall appoint one member of the Board to serve as a liaison to the PRC.
The bill repeals the provision requiring the Health Claims Arbitration Office to forward allegations requiring further investigation to the Faculty, and stipulates that the Board shall enter into a written contract with an entity or entities for further investigation and physician peer review of allegation (formerly a function of the MEDCHI).
Following an allegation of grounds for disciplinary or other action, the Board may refer the allegation for further investigation to the entity that has contracted with the Board. Before the Board takes any action following the investigation, it shall give the individual against whom the action is contemplated an opportunity for a hearing
before a hearing officer or a subcommittee of the Board. In conducting a case resolution
conference, the Board must provide an opportunity for the licensee who has been charged and the individual who has filed the complaint to appear before the Board. Peer review activities must be conducted by two reviewers, and in the event of lack of agreement between the two, a third reviewer must be used to render a final peer review decision. The affirmative vote of a quorum of the Board is required prior to exoneration of charges if the Board finds no grounds for action.
This bill authorizes the Chairman of the Board to delegate authority to conduct a hearing to a subcommittee consisting of three or more Board members. It also repeals the provision that factual findings will be supported by clear and convincing evidence, except in cases where the charge has failed to meet appropriate standards of care.
Previously the Board was required to create an individual profile on each licensee. The bill additionally requires that the Board maintain the profile for public use and include the following added information:
1) a copy of the public order with a description of any action taken against a licensee,
2) the number of medical malpractice final court judgments and arbitration awards against a licensee within the most recent 10-year period, for which all appeals have been exhausted as reported to the Board,
3) the number of medical malpractice settlements involving the licensee, if there are three or more, with a settlement amount of $150,000 or greater within the most recent five-year period,
4) a description of a conviction or entry of a plea of guilty or nolo contendere by the licensee for a crime involving moral turpitude reported to the Board,
5) medical education and practice information about the licensee, and
6) a statement on each licensee's profile of information to be taken into consideration by a
consumer when viewing a licensee's profile, including factors to consider when revaluating a licensee's malpractice data.
The Board will be required to maintain a website that serves as a single point of entry where all physician profile information is available to the public on the Internet. The Board must provide a mechanism for the notification and prompt correction of any factual inaccuracies in a licensee's profile.
The Board will be required to report to: the Governor, the Senate Education, Health and
Environmental Affairs (EHE), Budget and Taxation Committee (B&T), House Health and Government Operations (HGO), and Appropriations Committee (APP) by December 1 of 2003, 2004 and 2005 on the bill's changes to the licensure and regulation of physicians and other allied health professionals.
In addition, by January 1, 2004, the Board shall report to the Governor, EHE and HGO on investigative caseloads. The Board and the Office of the Attorney General shall also report on January 1, 2004, on all aspects of the Board investigative processes.
The bill also requires that investigations and peer review allegations shall utilize two peer reviewers, and in the event of a lack of agreement between the two reviewers, a third reviewer shall be utilized.
Contingent upon the Governor's including in the budget for FY 2005 at least $750,000 for the operation of the Health Manpower Shortage Incentive Grant Program and the Loan Assistant Repayment Program, effective July 1, 2004, these two programs will no longer be funded through the Board of Physicians.
For more information, please contact:
Sheila Higdon
SB0687
Health Maintenance Organizations - Patient Access to Choice of Provider
This law allows a Health Maintenance Organization (HMO) enrollee to select either a primary physician or certified nurse practitioner (CNP) as their primary care provider. If the enrollee chooses a CNP, that CNP must be at the same location as the nurse practitioner's collaborating physician, and the collaborating physician providing the
continuing medical management as required. Any enrollee that chooses a CNP as their primary care provider must be given the name and contact information of the collaborating physician.
The law also states that the language is not intended to require an HMO to include nurse practitioners to the organization's provider panel.
Effective Date: October 1, 2003
For more information, please contact:
Nicole Xander
SB0734
Health Occupations - State Board of Social Work Examiners - License
This law permits a social worker who is licensed in another state, or who possesses social work qualifications in another jurisdiction comparable to what is required in Maryland, and who has an application for licensure in Maryland pending before the Board of Social Work Examiners and meets regulations adopted by the board, to practice social work in Maryland for up to six months.
Effective Date: October 1, 2003
For more information, please contact:
Nicole Xander
[ Go to top]
Health Insurance
During the 2003 Session, the Legislature continued to examine ways to ensure accessible and affordable health insurance for Maryland citizens. While several bills were introduced, such as a proposal by the Maryland Citizens' Health Initiative to expand access health insurance, due to the tremendous budgetary crisis in the State, no new state funded initiatives were adopted. In an effort to assure that health care insurance in Maryland remains affordable and adequate, the Maryland Health Care Commission will conduct an evaluation of mandated health insurance services (HB605 - summary below). By January 2004, the Commission will make recommendations on existing mandated benefits, including decision-making criteria for reducing the number of mandates.
The State attempted to adopt HB753 to increase funding for the Medicaid program by subjecting Health Maintenance Organizations (HMO) and Medicaid Managed Care Organizations (MCOs) to the 2% premium tax. Currently, these plans are the only health insurance products not subject to the tax and by levying the tax on both products the State would be able to increase its share of federal matching funds for Medicaid. The business community opposed the HMO premium tax believing that the tax will increase health insurance costs, thus reducing access to affordable coverage.
In the area of health insurance, the most notable issue is the adoption of SB772/HB1179 - Nonprofit Health Service Plans Reform, which codifies the nonprofit mission of BlueCross and BlueShield of Maryland (see summary below).
HB0335
Community Access Program Grants - Coordination of Health Care Providers Reimbursements
The act authorizes recipients of the federal Community Access Program grants to establish pilot programs to coordinate health care provider reimbursements.
The pilot program is to enroll participates who are uninsured with incomes at or below 300% of the federal poverty level. The pilot is to coordinate the provision of health care services and provide payments to participating providers. The bill clarifies that payments by the pilot program are based on the availability of funding to the pilot
program. If a provider chooses to no longer participate in the pilot, they are required to
provide at least 30 days notice before discontinuing services. In addition, if the pilot reduces or discontinues benefits, they are required to provide at least 30 days notice to enrollees and employers of enrollees participating in the pilot.
The act states that the pilot created under this section is not an insurance product and is not therefore subject to regulation by the Maryland Insurance Administration.
The pilot program is to report to the Senate Finance Committee and House Health and Government Operations Committee before June 1, of each year on:
1) financial status of the pilot program,
2) data on the number of health care providers reimbursed,
3) description of the enrollee services utilized, and
4) other information requested by the committee.
Effective Date: July 1, 2003 (Sunset June 30, 2005)
For more information, please contact:
Jim Kaufman
HB0410
Health Insurance - Private Review Agents - Examination of Pharmacy Benefit Managers
This law requires the Insurance Commissioner to conduct an examination of any Pharmacy Benefit Manager (PBM) registered as a private review agent, to determine whether the PBM is acting in compliance with the law.
The examination shall be conducted every three years, paid by the person being examined. The Insurance Commissioner must submit a copy of the final report of the examination to the Senate Finance Committee and the House Health and Government Operations Committee within 30 days of the completion of the final report.
Effective Date: October 1, 2003
For more information, please contact:
Nicole Xander
HB0605
Maryland Health Care Commission - Evaluation of Mandated Health Insurance Services
This bill repeals the mandate that the Maryland Health Care Commission (MHCC) must determine the cost of mandated health insurance service, and evaluate the financial impact of each mandated benefit. Instead the MHCC must evaluate existing mandated health insurance services, and make recommendations to the General Assembly regarding decision-making criteria for reducing the number of mandates or the extent of coverage.
By January 1, 2004, and every 4 years thereafter, the MHCC must report on their evaluation of the following to the General Assembly:
1) assessment of the full cost of each existing mandated benefit as a percentage of the State's average annual wage and of premiums for the individual and group health insurance market,
2) assessment of the degree to which mandated benefits are covered in self-funded plans, and
3) comparison of mandated benefits provided by the State to those provided in Delaware, District of Columbia, Pennsylvania, and Virginia.
Effective Date: July 1, 2003
For more information, please contact:
Sheila Higdon
HB0700
Health Insurance - Private Review Agents - Certification
This Act authorizes the Insurance Commissioner to consider an applicant as having met certification requirements to become a private review agent if:
1) the applicant has obtained utilization management accreditation from an approved accrediting organization as determined by the Commissioner,
2) the approved organization has requirements that meet or exceed requirements, and
3) the applicant meets or exceeds requirements.
The law also requires the Commissioner to make available to the public on request, a report of an approved accrediting organization used by the Commissioner as evidence that the private review applicant has met the requirements to become a private review agent.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
HB0729
Health Insurance - Behavioral Health Care Services - Reports
The Act requires a carrier that contracts with an Managed Behavioral Health Care Organization (MBHCO) to include information on behavioral health care providers in the list of providers on the carrier's provider panel; and provide to enrollees upon initial enrollment the same information on behavioral health care providers as is required for other types of providers.
The law also extends the definition of "managed behavioral health care organization" to include a private review agent. In addition, the law repeals the definition of "mental health expense ratio." A carrier that contracts with a MBHCO must require the MBHCO to provide an annual report on the MBHCO's direct behavioral health care expenses. Direct behavioral health care expenses do not include behavioral health care
administrative expenses. The Act repeals the requirement that each carrier that provides behavioral health care services through a company it owns or through a contract with an MBHCO must report by March 1, to the Insurance Commissioner regarding the mental health expense ratio for the provision of behavioral health care services to members.
Instead, the carrier must complete and maintain a form developed by the Insurance Commissioner that must include:
1) the direct payments for the preceding calendar year;
2) information on the MBHCO's direct behavioral health care expenses; and
3) the carrier's total expenses for quality assurance and utilization management activities and treatment plan reviews that are clinical in nature. Each carrier required to complete and maintain copies of the forms must make them publicly available to an individual, enrollee, or member upon request.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
HB0894
Health Insurance - Reimbursement for Provider Services - Professional Counselors and Therapists
This law requires that if an insurance policy, contract, or certificate awarded by an insurer or a nonprofit health service plan provides for reimbursement of a service that is within the lawful scope of practice of a licensed clinical professional counselor, licensed clinical marriage and family therapist, or licensed clinical alcohol and drug counselor, the insured or any other covered person is entitled to reimbursement for the service.
Effective Date: October 1, 2003
For more information, please contact:
Nicole Xander
HB1100
Maryland Health Insurance Plan - Board of Directors
This act makes several changes to the Maryland Health Insurance Plan (MHIP) to include expanding the definition of "medically uninsurable" to include an individual who is eligible for the tax credit for health insurance costs under the federal Internal Revenue Code. The act also expands the membership of the Board of Directors of MHIP to include a representative of a carriers and an insurance producer selling insurance in the State.
The act, also requires a carrier that issues Medigap policies in the State to issue a policy to an individual eligible for Medicare if:
(1) the individual is enrolled under an employee welfare benefit plan proving health benefits and the plan is terminated,
(2) due to the individual's eligibility for Medicare, the individual is not eligible for the tax credit for heath insurance costs under the Internal Revenue Code,
(3) not eligible for enrollment in MHIP, and
(4) the individual applies for a Medigap policy no later than 63 days after the employee's
welfare plan terminates.
Beginning December 1, 2003, and annually thereafter, MHIP must report to the Governor and General Assembly on the number of members enrolled in the plan that is subject to the federal tax credit and these members associated costs.
Policy Note: In February 2003, International Steel Group, Inc. announced its intention to purchase Bethlehem Steel, which filed for bankruptcy in 2001. Prior to the acquisition announcement, Bethlehem Steel announced that as of March 31, 2003, it would terminate health and life insurance benefits for retirees and dependents, impacting almost 20,000 Baltimore area retirees. This bill was modified to allow Bethlehem Steel retirees to qualify for health care benefits through MHIP or access Medigap policies.
Effective Date: Emergency Measure (effective upon enactment)
Signed by the Governor on April 8, 2003; Chapter #2
For more information, please contact:
Nicole Xander
HB1179
Nonprofit Health Service Plans - Reform
The intent of this Act is to regulate the formation and operation of nonprofit health service plans in the State of Maryland, and to promote their existence. The mission of the plan shall be to provide affordable and accessible health insurance, assist and support public and private health care initiatives, and promote the integration of a statewide health care system.
The bill also establishes a Joint Blue Cross and Blue Shield Oversight Committee, that will require a nonprofit health service plan to report quarterly (beginning on December 1, 2003 and continuing through June 30, 2005) on its compliance with this act and other agreed upon information as outlined by the Committee. Beginning on
December 1, 2005 and annually thereafter, the Insurance Commission is to report to the Governor and General Assembly on the plan's compliance.
In addition to allowing a nonprofit health plan to satisfy the public service requirement by increasing access to or the affordability of health insurance, the act adds three new provisions for the public service requirement:
1) provide financial or in-kind support for public health programs;
2) employee underwriting standards that increase the availability of one or more health care service; or
3) employee pricing policies that enhance the affordability of health care services or products, that results in higher medical loss ratios than that of established comparable for-profit health plans.
The act also requires the non-profit health plan to administer and subsidize the Senior
Prescription Drug Program
and to offer a comprehensive benefit, open enrollment product in the individual market and small
group market.
The act states that the principle function of the 23 member Board of Directors shall ensure
the corporation
carries out the nonprofit mission, selects and evaluates corporate management, and ensure
sufficient resources
are available to meet the corporations objectives. The 23 member board is to include:
1) two individuals who will be non-voting members appointed by the presiding officers
of the General Assembly,
who are not members of the legislature;
2) no more than four members may be licensed health care professionals, hospital administrators,
or employees
of health care professionals or hospitals.
The Board chairman is to select a chairman for each board committee and the act stipulates
seven committees
to include an audit committee and a compensation committee. Board approval is required for any
action of the
plan and language was added stated that a decision by the board to convert to a for-profit entity
may be rejected
by any three members of the board.
Board members, who may serve a maximum of six years or two three year terms, may receive
compensation, in
addition to ordinary and necessary expenses, not to exceed $12,000 annually for members and
$15,000 for the
Chairman. The employees, executives, officers, and directors may only receive reasonable
compensation in the
form of bonuses, salary, or perquisites for work. To determine reasonable compensation, the
Board's
Compensation Committee is to develop guidelines based on similar non-profit health plans, in size
and scope,
operating in the United States. The proposed guidelines are to be submitted to the Insurance
Commissioner for
review and approval by June 1, 2004. The Commission shall have 60 days to review and take action
on the
guidelines or they will be considered approved. Furthermore, on an annual basis, the Commission
is to review
compensation paid by the plan. This section also applies to agreements for termination,
severance, bonuses,
and supplemental retirement benefits entered into on or after January 20, 1995.
The act creates the 17-member Joint Nonprofit Health Service Plan Oversight Committee,
appointed by the
President of the Senate and Speaker of the House, who shall appoint a Senator and Delegate to
serve as Co-
chairs. The membership of the committee shall be:
1) two members of the Senate,
2) two members of the House of Delegates,
3) the owner of a business that employs more than fifty people,
4) the owner of a business that employs two to fifty people,
5) a representative of a Maryland labor organization,
6) a member with experience in nonprofit administration and operation,
7) a representative of the State Employee Health Benefit Plan,
8) a representative of a nonprofit health care advocacy association,
9) a representative of the Medical and Chirurgical Faculty of Maryland,
10) a representative of the Maryland Hospital Association,
11) a representative of the Mid-Atlantic Association of Community Health Centers,
12) a third party administrator,
13) an insurance producer, and
14) two members of the public.
The act removes 10 members of the current board of directors by December 1, 2003. These
members are to be
replaced by a nominating committee, appointed by June 1, 2003, comprised of nine members. The
Governor,
President of the Senate, and Speaker of the House shall each appoint three members which will
comprise the
nominating committee. Each of the three appointments is to include one consumer member and may
not include
more than one health care provider. A member of the nominating committee may not be a candidate
for board
membership. Two additional board members shall be removed by June 1, 2004 while board members
representing corporations not subject to Maryland law shall be replaced by March 31, 2006. After
the 10 members
are replaced by December 1, 2003, the Board's Nominating Committee will choose all other board
members.
For a period of five years, a person may not file an application for the acquisition of the
plan and the Insurance
Commission may not approve an application for acquisition.
Language was included allowing the act to be severable. If one section is deemed to be
invalid for any reason,
the remaining sections will remain in effect.
Effective Date: Emergency Measure (effective upon enactment)
For more information, please contact:
Jim Kaufman
SB0039
Health Insurance - Coverage for Home Visits After Mastectomy or Surgical Removal of a Testicle -
Extension of
Sunset
The Act extends the sunset provision until September 30, 2006, for insurance coverage for home
visits following
a mastectomy or surgical removal of a testicle.
Effective Date: October 1, 2003
Signed by the Governor on April 22, 2003; Chapter #59
For more information, please contact:
Sheila Higdon
SB0148
Health Insurance - Medical Clinical Trials - Reporting Requirements
At the request of the Maryland Insurance Administration, this Act repeals the requirement that
health insurance
providers submit a report to the Insurance Commissioner that describes the clinical trials
covered during the
previous year, and repeals the requirement for the Commissioner to provide a summary annual
report to the
General Assembly.
Effective Date: June 1, 2003
Signed by the Governor on April 8, 2003; Chapter #15
For more information, please contact:
Sheila Higdon
SB0477
Small Business Health Insurance Affordability Act
This law allows insurance carriers to offer benefits in addition to the Standard Plan if the
benefits are offered and
priced separately, do not duplicate benefits, and the carrier clearly distinguishes the Standard
Plan from other
offerings of the carrier, indicates the Standard Plan is the only plan required by State law, and
specifies that all
enhancements are not required by State law. The Maryland Health Care Commission (MHCC) shall
exclude or
limit benefits or cost-sharing arrangements of the Standard Plan if the average rate for the Plan
exceeds 10% of
the average annual wage in the State.
By December 2003, the MHCC shall prepare a report on the methodology used in developing the
Comprehensive
Standard Health Benefit Plan in the small group market and the feasibility of creating a Basic
Plan in addition to
the Standard Plan.
The Maryland Health Care Commission (MHCC), in consultation with the Insurance Administration,
shall conduct
analysis and make recommendations on the administrative cost of health plans in the small group
market by
January 1, 2004.
Effective Date: July 1, 2003
Signed by the Governor on April 22, 2003; Chapter #93
For more information, please contact:
Nicole Xander
SB0672
Health Insurance - Provider Panels - Lists of Providers
This Act alters the manner in which health insurance carriers are required to provide to
enrollees and prospective
enrollees, a list of providers on the carrier's provider panel. Carriers will be required to
inform each existing and
prospective enrollee how to obtain provider information on the Internet or in printed form.
Effective Date: October 1, 2003
For more information, please contact:
Sheila Higdon
[ Go to top]
Higher Education
Johns Hopkins, along with MICUA, advocates on multiple legislative initiatives in the higher education sector, but due to the State's fiscal challenges, the number was down over 60% from previous years. Bills designed to strengthen higher education in Maryland's were supported, including legislation aimed at alleviating the State's shortage of teachers and others lessening the costs of higher education for students. One bill that failed that we strongly supported was Senate Bill 291, which would have allowed a recipient of a Maryland Teacher Scholarship to perform the required service obligation as a teacher in a nonpublic elementary, or secondary school that holds a certificate of approval from the State Board of Education. Many teachers start out in the parochial or private schools, and when they have gained the necessary experience, move on to the public system where the pay, promotions, and opportunities are greater. Johns Hopkins believed that making it easier for these individuals to start teaching would ultimately result in a greater proportion of teachers moving into the public system after they have gained some experience in the nonpublic schools. We believed this was one way to help
bring more teachers into Maryland to help the teacher shortage crisis.
Another higher education priority for Johns Hopkins was SB555 which would have reduced the State's aid to nonpublic institutions of higher education by altering the methodology for calculating the full-time equivalent (FTE) student count that is used to determine aid under the Joseph A. Sellinger formula. FTE counts for in state and out-of-state students at each institution would have been computed separately, and the out-of-state FTE student enrollment would have been reduced by 25%. The Sellinger aid formula for each institution would have been calculated using the reduced FTE computation. For Johns Hopkins, the bill would have resulted in a $3.1 million reduction in next year's Sellinger Aid formula and lowered appropriations every year thereafter. With the assistance of MICUA, this bill received an unfavorable report from the Senate Budget and Taxation Committee.
House Bill 568 would have authorized Senators and Delegates to award all or a portion of the funds authorized for the Senatorial or Delegate scholarships to a public institution of higher education or an academic program in a public institution of higher education. This bill would have required the public higher education institutions to award the scholarships to only residents of Maryland. Johns Hopkins and MICUA attempted to amend the legislation to allow a legislator to award a Senatorial or Delegate scholarship to individuals who intend to study and work in a workforce shortage area in Maryland, including nursing and teaching. The proposed amendments attempted to encourage legislators to provide needed financial aid to students willing to study and work in these critical workforce shortage areas. This bill however did not pass.
HB0030
College Savings Plans of Maryland
House Bill 30/Senate Bill 499 changes the name of the Maryland Higher Education Investment Board
to the
College Savings Plan of Maryland Board, and establishes the title of the College Savings Plan of
Maryland for the
two programs that are administered by the Board. These bills also clarify that tuition charges
covered by the
program include only the actual tuition and mandatory fees assessed to all students as a
condition of enrollment.
These bills allow the Board to combine the required annual audits and reports for the Maryland
Prepaid College
Trust and the Maryland College Investment Plan and make other technical changes in order to align
the
administration of the two programs.
Effective Date: July 1, 2003
For more information, please contact:
Bret Schreiber
HB0253
Higher Education - Resident Tuition Charges - Immigrant Students

