 FIFTY YEARS AGO, nobody knew how many chromosomes the human body
has. Today, it's agreed that all human genetic sequences will be
deciphered by the year 2002, maybe sooner.
FIFTY YEARS AGO, nobody knew how many chromosomes the human body
has. Today, it's agreed that all human genetic sequences will be
deciphered by the year 2002, maybe sooner.
FIFTY YEARS AGO, nobody knew how many chromosomes the human body
has. Today, it's agreed that all human genetic sequences will be
deciphered by the year 2002, maybe sooner.
One reason could be Hopkins geneticist Victor McKusick (MD '46) and a quiet little institution he co-founded 37 years ago--the annual Short Course in Medical and Experimental Mammalian Genetics, which I attended this past July.
"What did you do on your summer vacation, Mom?" "I went to the Jackson Laboratory at Bar Harbor, Maine, where I went to lectures from 8:30 to 12:30, plus afternoon workshops and evening lectures. The air was redolent of pines and mice, from the thousands of experimental mice bred, kept, and sold by the Jackson Lab, otherwise known as the Mouse House, and the two weeks were as crowded as this sentence. It was great."
"Well, didn't you even do any hiking?" "Yes, on Saturday afternoon and Sunday, if it wasn't raining."
"And this was fun? Mom, you're weird."
"Well, we did go out to dinner every night, before the evening lecture."
ACTUALLY, in this particular group, what would have been weird was goofing off. Admission to this course is competitive, and people came from around the globe expressly for this quick yet comprehensive overview of genetics at the forefront. So while the setting might be shorts-and-volleyball, the faculty comprised a healthy portion of the international A-list in medical genetics (including some from Hopkins). They were assembled to give us the very latest word on their field--what McKusick calls "everything medical about genetics, and everything genetic about medicine"-- and all we had to do was lap it up. Obviously, we would hike some other time.
The 111 students were of all ages, from grayheads to a few undergraduates and high school students who were research interns at the Jackson Lab. We came from universities and medical centers; from the CDC, NIH, and FDA; from 10 major drug companies and 14 different countries. There was even a separate track in which science writers from places like Newsweek, Newsday, and The Scientist got their own special lectures. (I dropped in on them, but mostly stayed with the Short Course itself.)
About a third of the Short Coursers were PhD researchers, another third physicians. Many were authorities in some genetic specialty, lured by the promise of new ideas from other areas. Of the rest, the biggest group was graduate students, plus a few computer jocks who came to learn what scientists need in a database. Several college professors were preparing to teach genetics. In short, it was a more or less typical group of Short Course students: heterogeneous and serious.
In the early days, says McKusick, before genetics had become established as an important part of clinical medicine, "we also got a lot of medical deans. They came to see"--he mimicks, only slightly ponderous--"'what we ought to be doing about genetics.'"
Yes, this course is influential. That the deans came speaks for the content, and also has to mean that the Short Course helped shape today's teaching and practice of medical genetics. A majority of the field's leading researchers, including departmental chairs, have passed through this course as students, faculty, or both.
But don't get me wrong. The beautiful coast of Maine is "not a deterrent," as one woman said.
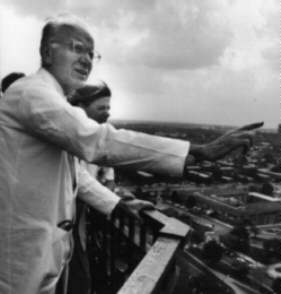
THE COURSE IS Victor McKusick's baby--one of them. He has been physician-in-chief (and William Osler Professor of Medicine) at Hopkins for 12 years; founder of Hopkins's Center for Medical Genetics; creator of the first major genetic database; a founder and first president (1988-90) of the Human Genome Organization, the international organization that helps coordinate genetic research worldwide; and the author or co-author of some 15 classic reference texts.
The Short Course seems to be one of his favorite children, however. At Hopkins, he can seem distant, a man who always wears his long white coat. In Maine, though he retains his jacket and tie, he puts on white sneakers and plaid pants and a big smile. He takes particular care to talk with the younger students.
McKusick co-founded the Short Course with Earl Green, then director of the Jackson Laboratory, and today, 37 years later, he is still co-director. It is still he who gives the first day's opening lecture, a history of medical genetics crammed into 45 minutes. It is still he who rings each day's opening bell (a Swiss cowbell) at 8:30 sharp, he who introduces the speakers. At each and every lecture, he folds his tall, somewhat lanky frame into a seat at the far left of the front row, his straight back and his white head somehow radiating attentiveness through the room. He sets the tone.
Over the years, McKusick says he has insisted that "we always start from first principles." Accordingly, the faculty started with basics, whiffing whole specialty courses past our nose in half an hour. "Codons, introns, exons, transposons, got that? Now we'll talk about mitochondrial DNA." (That's an exaggeration, but not by much.) Then they'd sprint on to new, not-yet-published, hot-stuff techniques and findings, marked by a sudden flurry of note-taking.
It was heady stuff, even the "basics," even for someone who's been writing about genetics since 1983--and also profoundly disorienting, because when it was all over, I found I'd passed like Alice through some sort of mental spacewarp Wonderland.
This intellectual world looked familiar--chromosomes, patients, mouse models, sequencing and mapping genes, etc.--and nothing I'd ever written on medical genetics was actually wrong. Yet my presuppositions were out of kilter; it was as if I'd been diligently writing about leaves while the forest moved. So I can tell you that much of what "everybody knows" about medical genetics turns out to be wrong, irrelevant, or passe. For example:
Yet researchers seem confident. "Multifactorial used to be a code word for 'we'll never get that,'" one Hopkins geneticist told me. "Now we're expecting to find at least the heavy hitters [among the genes]."
The question is valid, if broad (and perhaps hypocritical, in a system that already denies much care to the indigent). Nevertheless, it was not so much as mentioned in the Short Course.
I think that's largely because the context is so medical. Most of my classmates at the Course were (or will be) basic researchers. When they leave their labs, however, many put on white coats and see patients. So while they enjoy intellectual puzzles, their ultimate concern is not puzzles or spreadsheets or moral abstractions. Their driving concern is individual, suffering people, whom they see in the flesh, one at a time.
At the Short Course, I, too, saw patients, some at a clinic but most in slide after slide after slide: sisters all of whom have cancer. Children with Prader-Willi syndrome, achondroplasia, various kinds of mental defects. Children born with no brain. Children smiling gamely at the camera, despite their spindling legs. Some 6 percent of human infants are born with major congenital malformations.
The heart sinks in the face of so much suffering, even when it's only seen on slides. When it's seen in person, the only reaction can be, "Stop talking, let's just get on with it. Maybe we can't help everyone, but let's do what we can do." The feeling can amount to a kind of fury.
What medicine can do, at this point, does not include gene therapy. Human genetics are complicated beyond belief, and so far, less than 5 percent of the human genome has even been sequenced. It's true that what's known includes some of the most medically important disorders. Nevertheless, the speakers said that most clinical trials of gene therapy are premature. We're not there yet.
Even when we do get there, it's thought that most therapies will not actually change the faulty genes. A few will introduce long-lived cells having normal genes, which can provide the normal proteins a patient's body has been lacking. (See "Stalking the Stem Cell," June 1996, Johns Hopkins Magazine.) For example, there's been some early success using stem cells to treat severe combined immune deficiency (SCID), the disease of the former "bubble children."
Most new treatments, however, will be genetic only in the sense that they will arise from genetic research, with its precise new understanding of fundamental body chemistry. In that sense, gene therapy is already here. Several speakers mentioned--smiling, they like these--diseases like PKU, phenylketonuria, a formerly devastating genetic disorder that is now largely controlled by diet.
Overall, progress toward cures will be slow and incremental. David Valle, a Hopkins geneticist/pediatrician who also co-directs the Short Course, told us that in 1985, of patients with the known genetic diseases, physicians were able to cure 12 percent and produce improvement in 36 percent. In 1995, those numbers stood at 12 percent and 47 percent--better, but hardly radical change.
"I think the greatest hope will be for patients with multifactorial disease," said Paigen. (Once that multifactorial disease is somewhat understood.) That's because if it takes 10 factors to cause outright disease, maybe correcting any one or two will be enough to eliminate symptoms. Devising those treatments should be a lot easier than cures for one-factor disease, where only the bull's-eye will do.
Each talk ended with a brief Q&A, in which the most usual answers were, "I don't know." "We don't know." "We have no idea whatsoever." "We're looking into that."
To non-scientists, such talk can sound like failure, ineptitude, and wasted money. But to scientists at the forefront, what they don't know delineates what they do know. It provides a marker, the limit of firm ground where they can stand, hang their toes over, and craft a new question. Don't-know marks the cutting edge.
If one knows the answers, after all, there's no point in research.
 FROM THESE TWO WEEKS I came back to Baltimore and went into
culture shock, because every time I'd pick up a paper or magazine
and read something about genetics, the material was almost
unrecognizable. I saw with new eyes that even respectable,
responsible science writers--myself, for example--were presenting
a science that was strangely tidy. All the facts were
unambiguous, all the experiments successful (at least the ones
described). All scientists were forging yet another link in the
chain that will Lead Humankind Into A Better Tomorrow, or so the
reader could infer.
FROM THESE TWO WEEKS I came back to Baltimore and went into
culture shock, because every time I'd pick up a paper or magazine
and read something about genetics, the material was almost
unrecognizable. I saw with new eyes that even respectable,
responsible science writers--myself, for example--were presenting
a science that was strangely tidy. All the facts were
unambiguous, all the experiments successful (at least the ones
described). All scientists were forging yet another link in the
chain that will Lead Humankind Into A Better Tomorrow, or so the
reader could infer.
And I got to thinking: No wonder the public (including Congress) is eagerly awaiting gene therapy. Every article implicitly makes that promise, simply by virtue of the format used for research reporting. Note that word "reporting." Science news is first of all news, meaning that if there's no news peg, there's no story: Something has to have happened.
Moreover, according to the rules of news, that something has to have meaning to the reader even before the reader reads. So we reporters always start at the us-humans level, and we don't tell you the infinite complexity of it all, the technical details. We rarely write about negative findings--that X, which looked so promising, appears not to work. We skip the don't-knows as too confusing (and anyway, not news). We leave out statistical methods and technical procedures unless someone hopes to make money on them.
The little that's left falls neatly into The Format, which goes as follows: An opening sentence or two that tells you why you want to keep on reading. In medical writing, this section almost always implies a clinical application. Then comes a brief review of the experiments and the evidence, and on to the ritual closer, which says, often in so many words, "While researchers caution that much more needs to be done, this work represents a significant step toward the time when"--here one fills in the clinical application--"will become reality."
In sophisticated, more feature-type coverage, like that of The New York Times, you'll get more details on the experiment. Also reactions from other researchers, usually one pro and one con (the con leads naturally into more-work-to-be-done). You may even get a substantial discussion of what that remaining work will be, before the significant-step-forward.
The plot-line, however, never changes, and it has a suspicious likeness to the Hero's Journey, in debased form. Instead of the Grail, we have the Cure. The Black Knight transmogrifies into a spokesman for con, the Forest of Thorns into an intellectual thicket. Otherwise, it's your basic quest in the face of adversity. Science is told as heroic adventure, to help people relate to it.
And that's good. It works. Yet I find myself concerned. There has to be an impact when we read, again and again and again, that new advance A, despite B, should give rise to C. (Imagine trumpets in the distance.) Does this way of presenting science make us too complacent? Too certain that technology can overcome all problems? Does presenting science as the hero's quest reinforce the false premise that the way is always forward, always open?
I think so, and I wonder what will happen when gene therapy doesn't come along on the heels of the full genetic sequence. Funding could dry up, too soon, in a backlash. Might research money vanish just when some success really was in reach?
YET, PARADOXICALLY, I came away from the Short Course with lots of hope for applications, even in the fairly short haul, and I found it in precisely those areas we reporters do not cover: in the dull-sounding techniques, procedures, statistical methods, and databases--which are coming along very nicely, thank you.
At lunch one day with a faculty member, I was startled to infer that, in principle, once you've sequenced a gene, you can figure out what it does. Not easily, but you can. And that conversely, once you have a trait, you can isolate the gene.
I sat up straight. Wait a minute, I said. Do you mean to tell me that you can go both ways? Yes, he said, impatient, waiting for some better question. (Surely I knew that.)
No, I didn't, and I don't think most of the public does. In other words, researchers now have the technology to answer almost any question you'd like to ask about medical genetics. Granted, there are millions of questions. The actual experiments are extremely difficult and time-consuming. In many cases, even with full knowledge, cures may be impossible.
That said, it remains true that in the '90s, a full panoply of genetic tools has developed. To me, medical genetics looks to be at the point computer scientists reached once they had the silicon chip and fiber optics. There's a way to go, but the groundwork has been laid.
So, what are these genetic tools? One whopper is the result of techniques that fool yeast and bacteria into thinking a piece of human DNA is part of their own DNA, so that they preserve and reproduce it. These bacteria and yeast--called BACs and YACs (for bacterial artificial chromosome and yeast artificial chromosome)- -constitute living libraries of human DNA, which can be manipulated. Researchers can now order, for example, a YAC of human chromosome 6.
The first complete YAC library, which holds overlapping clones of the entire genome in large but workable chunks, appeared in 1993. BACs hold smaller chunks than YACs but are more stable; most agree they will be the workhorse of the Human Genome Project.
A second major tool is PCR, the technique of polymerase chain reaction, for which Cary Mullis won the Nobel Prize in 1993. "It's the most important thing in DNA research in the last two decades," says John Schimenti (he's a mouse researcher and the Course co-director from the Jackson Laboratory), for reasons Norman Arnheim of USC explained: "PCR lets you amplify the needle"--genetic material--"so much it dominates the haystack."
Now that the technique has been fully developed, researchers can multiply specific segments of DNA until they really have enough to work with, not in days but in hours. They can isolate a very small segment of gene very rapidly, then clone it, make probes from it, and use those probes to fish out and identify adjacent sequences of DNA. Students at the Short Course had a workshop on the nitty-gritty of PCR, as well as several lectures on how-tos and applications--applications like these:
 ALONG WITH PCR, the genetics of yeast and mice are both steaming
hot areas for research. They matter to medical genetics because
other genomes serve as a window on the human one.
ALONG WITH PCR, the genetics of yeast and mice are both steaming
hot areas for research. They matter to medical genetics because
other genomes serve as a window on the human one.
Imagine yourself as a researcher on the genetics of an enzyme or a membrane protein, and you've just sequenced a gene that seems to have some bearing. But what the devil does the gene do? To find out, it is newly possible to go to the genomes of other organisms and look for homologues, similar sequences that may serve a similar purpose in humans. If the homologue's function is understood in the non-human genome, you've got a really useful lead. (Probably.)
Take yeast, for example. Geneticists do, with enthusiasm, because it's the simplest and best model for animal cells: Yeast is a single-celled organism with a lean, mean 6,000 genes. (People, by contrast, have 80- to 100,000.) Yet that 6,000 is enough to handle all the fundamental chemistry an animal cell needs to live and reproduce. Furthermore, yeast cells work much the same way as cells in more complex creatures.
The yeast and human genomes parted company about a billion years ago, Philip Hieter told us. (He's a molecular biologist and geneticist at Hopkins medical school.) Yet because evolution tends to conserve any system that works, the similarities are powerful. Yeast cells have mitochondria, vacuoles, golgi apparatus, a doubled membrane around the nucleus, and more: "all the basic processes [of cell metabolism]," in Hieter's words.
As of April 24, 1996, yeast--S. cerevisiae--has been fully sequenced. Now the puzzle has no missing pieces, and all the data are freely available to the public, including data on the genes whose function is now understood. That completeness lends assurance as researchers compare the yeast genome with others by means of a Web site at http://genome- www.stanford.edu/Saccharomyces. The site is currently getting nearly 50,000 hits a week from researchers around the world.
That's how the genetic defect involved in cystic fibrosis was figured out: clues came from the CFTR gene in yeast, revealing the precise role of CFTR in a cell's sodium transport. More recently, the defect for ataxia-telangiectasia, a fatal degenerative brain disease in children, was deciphered by means of a five-minute computer hunt. It turns out the sequence is biochemically related to yeast enzymes critical for cell growth and DNA repair. Such speed seems ironic, because it had taken 18 years to assemble enough affected families, then to find and clone the gene, said Mark Boguski, director of the new National Center for Biotechnology Information (NCBI) at the National Library of Medicine. He quoted David B. Wake: "Homology... is the central concept for all of biology."
Mice are closer to people than is yeast, the genomes having parted a mere million years ago. So mice can be used to look at body chemistry on a larger scale, as in organs, fetal development, or interactions among different types of cells and chemical reactions. Then once researchers understand a particular system, mice can also be used to test out interventions. "Mice will give us prevention," said the Jackson Lab's Paigen. "They are the mammal of choice."
Mice make ideal experimental animals because they're cheap (one-tenth the cost of rats), they breed quickly, and they're easy to work with. Even if ethics allowed human experimentation, Paigen noted dryly, humans are poor test subjects. "People won't do controlled matings, they take too long to reproduce, and they are unwilling to be on special diets for months while their aorta is periodically examined."
Hence the need for experimental mice--mice that are genetically identical (it takes work to keep them that way) and available by the thousands and millions. The world's primary supplier of experimental mice is the Jackson Laboratory, a non-profit institution that breeds, collects, maintains, and sells some 120,000 varieties of mouse to labs all over the world, as well as continuing its own research.
Many of those mouse lines are used specifically to model human diseases. Diabetes, for instance, can be studied in the grossly obese db mouse.
Several of the lines at Jackson stand in for normals, however. One such is "Black 6," a mouse line that is more than 50 years old. By now, Black 6 chemistry is massively documented (if not always understood), so these old lines make an ideal background for new manipulations of the genome: knock-out mice, for example.
In this technique, developed in 1986, you knock out (inactivate) a particular gene or genes and see how the mice do, compared with their unaltered cousins. While results are unpredictable and difficult to interpret, many new insights are arising that way. For example, a recently developed line of knock-out mice burn brown fat differently. Therefore they stay healthily thin, even when they live on the mouse equivalent of Big Macs.
Researchers can also knock-in particular genes, even genes from other species. For example, mice have been engineered to have human immune systems. For research on infectious diseases, these mice are pearls beyond price.
So in general, with mice, geneticists can experiment away. They can come to understand (they hope) precisely how the body chemistry works, as dictated by genes, and can apply their understanding to people.
"We are not so different from a mouse as you might hope," said Paigen. Mice have much the same genes as humans, albeit arranged on 40 chromosomes instead of 46. "There was a primordial genetic structure that's suffered about 150 breaks and reshufflings," Paigen said. And that's why mice "get just about every disease we do." What's learned about mice, for the most part, applies to people and other mammals.
The mouse genome is clipping right along. Janan Eppig, a researcher at the Jackson Lab, told us that as of July 1996, 7,229 mouse genes are known; 5,201 of them have been mapped; and 1,772 have been matched to their human counterparts.
THE BEAUTIFUL PART is that starting in the '90s, the maturing Internet has made all this information freely available, with daily updates. Since the World Wide Web was established in 1993 and 1994, the Internet has become the newest, glossiest tool that geneticists have, because it allows them to prospect in one another's data. The Mouse Genome Database (MGD), for example, came online in 1994 and is maintained at the Jackson Lab by Eppig and her group, with support from NIH. You can reach it at http://www.informatics.jax.org
You should know that these academic databases, unlike commercial ones, are not proprietary. Currently, their use is free or costs at most a moderate subscription fee. Nor are they sleekly graphic, as you might expect from America On Line. Rather, they are structured strictly for function, to hold maximum data; from a scholarly point of view, it's far better to put in too much information than to risk leaving out a detail that might prove crucial.
So the databases are full to bursting, page after page of just-plain diagrams and text on such things as, for the MGD, a full description of all inbred mouse strains; plus primers used to fish for various locations in the genome; plus much, much more. From the MGD, geneticists can hopscotch over to the mouse sequence database and so on, moving from one linked database to another, all over the world.
All academic fields now use the Web in this way. For example, a resource that is general to all of medicine is MEDLINE, a database at the National Library of Medicine that presently contains 800,000 medicine-related abstracts from journals all over the world. Many doctors and all universities subscribe, so medical faculty can easily use it, and geneticists certainly do. Biological databases are all interlinked with relevant abstracts on MEDLINE.
The Web is not all positive: Sometimes information is missing because nobody ever put it in. Often it's there but hard to find. Sometimes it used to be there, but no one maintained the Web site so it disappeared. (The average lifespan of a Web site is six months.) Funding is scarce for databases, and what there is tends to support setting one up; maintaining and updating them lacks glamour.
Nevertheless, the genetic tools on the Web are a dazzling array, and most are in the committed care of institutions like the Jackson Laboratory, Johns Hopkins University, Harvard University, or the NCBI. (Its homepage at http://www.ncbi.nlm.nih.gov/ will lead you to most major biological databases.)
Besides MEDLINE and the genomes of yeast and mouse, key resources for medical genetics include:
That's the way it's going to be for geneticists in the next few years. In the course, Peter Goodfellow (lately of Cambridge University, now at SmithKline-Beecham) pointed out that genetic information is growing, not at an exponential rate, but at an exponential rate of an exponential rate. You can't graph it in the normal way: the line shoots straight up.
After many, many years of slogging progress, one hard-won bit of information accumulating after another, it seems that critical mass has been reached in medical genetics. The computer revolution has met the revolution in molecular biology, and look out Nelly.
THE SHORT COURSE'S GRAND FINALE, to my mind, was the final evening lecture, given by McKusick, with slides he's taken from the Course's very beginning. Now he loped back and forth, so enthusiastic he almost babbled as he stretched the pointer to persons of special interest. "Here's Virginia Apgar," he said. "You can always find her in a picture because of the white hair." Here was a young Leroy Hood (Hopkins MD '64), who was to develop key technology including the automated DNA sequencers. Here was a very young Clair Francomano, then a high school student interning at the lab, later a postdoc at Hopkins, now director of medical research at the National Center for Human Genome Research (and a faculty member at Hopkins and the Short Course). Here was a future Nobel laureate, George Snell. An already Nobel laureate, Daniel Nathans. A person who was to discover the fragile X syndrome, and more, more, more. It was a hail of names, faces, and accomplishments. "It's amazing," Valle said later. "There's this huge number of people who have made and are continuing to make major contributions in human genetics, who were students in this course."
Over the years, the faculty numbered 109 from the Jackson Laboratory, 82 from Johns Hopkins, 227 from elsewhere in the world. Students to date: 3,581.
As the names and faces rolled by, I began to imagine some of my bright-eyed classmates joining that proud gallery, in time. Surely some would be invited to become faculty, would belong on these lists of people McKusick is proud to have fostered. And as a group, I thought, between their medical care and their research, these people would help hundreds and thousands of patients who would never, ever, ever hear of the Short Course in Medical and Experimental Mammalian Genetics.
Then, with a thump, I came back to the present. It was time for warm Cokes and conversation in the lobby.
Elise Hancock is the magazine's senior editor.